


Omicron causes hospitalisation like previous variants
It also escapes infection-acquired and vaccine-induced prior immunity and is much more transmissible


It has only been a few days since an Irish W.H.O. meeting skipped two letters of the Greek alphabet and named the new Variant of Concern from southern Africa Omicron [WP]. Here at Nutrition Matters, [WP] denotes a link to the relevant Wikipedia page, where, for Omicron, we can see a radial lineage diagram depicting Omicron shooting off from a very early origin, in a totally different direction, from the spray of now hundreds of sub-types of the Delta variant.
We all know Omicron is highly transmissible, from its rapid spread, mainly in South Africa’s Gauteng province, now extending to its detection in at least 40 [WP] countries. (The number was 37 six hours ago when I started this aricle.) Community transmission outside Africa has been confirmed by a person being infected at a crowded New York City anime conference in which all participants had received at least the first of the two injections currently required for the recipient to be considered fully vaccinated.
Everyone knows that Omicron has an unprecedented number of mutations with respect to the original Wuhan SARS-CoV-2 virus. So there are well-justified fears that it will exhibit a high degree of immune escape [WP] - the ability to infect a person despite them mounting an antibody response due to potentially multiple types of immunity which they acquired from infection with a prior variant, from a vaccination, or from both of these in either order.
There has been a great deal of optimism that Omicron would cause less severe symptoms than prior variants, primarily or solely due to the reports from several highly qualified physicians in South Africa’s Gauteng province [WP] the relatively small inland province which encompasses Johannesburg and 15.8M of the country’s 60.1M people. Dr Angelique Coetzee’s comments can be found in a Telegraph article and in tweets linked to from this ZeroHedge article.
Before discussing Omicron’s ability to cause symptoms severe enough to warrant hospitalisation, and the first piece of research regarding its immune escape properties, here are some links to sites of interest to anyone who is keen to pursue the latest COVID-19 developments regarding early treatment and vaccine safety and efficiency. I have paid subscriptions to all these.
moderndiscontent.substack.com Deeply researched, careful, analysis of the most pertinent early treatments and biomedical matters.
roundingtheearth.substack.com Wide-ranging discussions, particularly about COVID-19 vaccine safety and efficacy, from math and statistical analysis specialist Matthew Crawford.
alexberenson.substack.com Alex Berenson’s Unreported Truths - an enormously popular (200k subscribers) Substack concerning the pandemic.
stevekirsch.substack.com Steve Kirsch funded research into COVID-19 early treatments and now devotes his monumental energies to COVID-19 vaccine safety problems. I keep trying to draw his attention to vitamin D, via this Substack and vitamindstopscovid.info. If you can help me achieve this, such as by writing comments to his articles, I would really appreciate it.
trialsitenews.com USD$5 a month for excellent articles with constructive, potentially long, comments and discussion groups such as on COVID-19 early treatment vaccines.
www.zerohedge.com Very popular doom-laden investment news site which goes well beyond stocks and bonds and into important social, political and health matters.
Omicron’s origins are a mystery
Detailed genetic data regarding SARS-CoV-2 variants can be found at www.gisaid.org/hcov19-variants/. A tree-like plot of the divergence of thousands of slightly different types of SARS-CoV-2 viruses can be found at: nextstrain.org/ncov/gisaid/global .
The best discussion I found of Omicron’s origins is this 2021-12-01 article by Kai Kupferschmidt: www.science.org/content/article/where-did-weird-omicron-come which begins with this graph, which was somehow made using the Nextstrain site and which depicts only the mutations in the S1 part of the spike protein:

From this we can discern:
Most of the dots, each representing one or more detections of viruses with a distinct genetic pattern, are classed within the three clades [WP] (not shown distinctly here) known as Delta.
The number of mutations in the S1 section of Delta genetic codes - each being a deletion, addition, or a change in one of the few thousand base pairs [WP] of the total ~29,303 base pairs in the whole genome - numbers between 3 and 15.
The Delta clades began differentiating in late 2020.
The number of S1 mutations in currently sequenced Omicron genomes is between 20 and 28. This is about three times as many as in Delta.
According to our best understanding of viral evolution, these Omicron genomes which have been sequenced so-far began diverging from an unknown common ancestor only two or three months ago.
That common ancestor is thought to be much the same as variants from April 2020.
This is very puzzling. It would be explicable if someone stored an early virus and then let it infect hosts (humans, or perhaps some non-human animals) a few months ago - but no-one seriously suspects this.
The Science article mentions various hypotheses of Omicron's origins, including evolving over months in an immunocompromised person (such as someone suffering from HIV) and evolving in a non-human species. There is no sign of consensus on which hypothesis best explains the observations to date.
Omicron's novel, highly mutated, genetic structure is unstable and is expected to evolve rapidly in divergent ways
Omicron’s genetic structure is thought to be unstable, in that it is not necessarily fine-tuned for optimal survival - though such evolutionarily fine-tuning can lead to hundreds or thousands of variations with somewhat lesser or greater survival benefits. This means it can be expected to evolve rapidly, and so perhaps develop even higher-performance viruses. We see this already in the 20 to 28 range of S1 mutations, in a clade which was discovered less than a month ago.
The theory that viruses tend to evolve to become less virulent need not apply
There is a well-known and generally valid theory that viruses, like bacterial and other types of pathogen, tend to evolve to be less virulent - to cause less severe disease, or even no symptoms at all.
The sole evolutionary pressure which selects for the survival of random mutations in the viral genome is the ability of the whole mutated genome to increase transmission, in whatever range of circumstances the viruses and their hosts find themselves in. One way a virus can increase its transmissibility is if it evolves to be at least as good as generating viruses to be sneezed, coughed or breathed out, while also reducing symptoms during its infectious phase so that the hosts go about their business normally and maintain high levels of interpersonal contact. (Viruses can also increase their transmissibility by changing host behaviour to increase physical distribution of the same number of viruses, such as by making people sneeze and cough, or by making dogs crazed and driven to bite other dogs and people, as is the case with the hideous disease rabies. [WP])
A great deal of hope has been invested in the idea that a SARS-CoV-2 variant will evolve which produces few symptoms, while being highly transmissible. This could be allowed to spread to most humans, as long as it also induced a lasting immunity which confers strong protection against infection (ideally) or (at least) severe symptoms from other more virulent variants.
There has been no evidence of this occurring, and today - 4th December, 2021 - I think it is fair to say that a large fraction of humanity is hoping that this is true of Omicron. Their hopes have been, somewhat reasonably, buoyed by the early reports from the South African doctors. Another, lesser known, source of support for this optimistic hypothesis comes from a 29th November analysis in French and English, by Professor Jaques Fantini, based on a technique he and his colleagues developed for quantifying (as a “T-index”) the transmissibility of a SARS-CoV-2 virus by using molecular simulation of the fit and electrostatic attraction between the two lobes of the viral spike protein and the ACE-2 receptor and other molecules embedded in the plasma membrane of our cells, which the virus has evolved to infect.
Prof. Fantini estimated that Delta’s predominance was due, in large part, to its T-index being 10.67, which is much higher than the 2.16 of the original Wuhan strain. He estimated the T-index of Omicron was just 3.90. He noted that “avalanche of mutations does not obey any selection logic” and that these will cause immune escape as pre-existing antibodies would not latch onto the Omicron spike protein so well. He concluded that Omicron would not supplant Delta, due to its low T-value.
However, in the early South African summer, with Delta infections declining rapidly to very low levels, Omicron has transmitted very rapidly indeed. There is not a high enough proportion of the population who have been previously infected or vaccinated for this to be due primarily to immune escape: existing immunity suppressing transmission of Delta and older variants, but not so strongly suppressing Omicron.
The doctors reporting only mild symptoms (though severe fatigue and children with racing hearts doesn’t sound mild to me) with no hospitalisations to date. However, they could observe this even if Omicron causes just as serious disease as Delta, for a number of reasons:
South Africa has a relatively young population. Serious disease and deaths take weeks to develop. The prevalence of Omicron is rising far more sharply than previous variants.
The truth of the matter takes longer to be discerned, and I am writing this article directly after first clearly discerning, to my own satisfaction, that Omicron does cause serious disease, much like the other variants, in typical populations who have disastrously low vitamin D levels and no access to early treatments.
We will get to the evidence for this serious disease in a few minutes. I am still preambling!
Since most people - doctors and public health officials included - have no clue that the COVID-19 pandemic would be suppressed to very low levels of transmission, harm, and death, by population-wide boosting of 25-hydroxyvitamin D to 50ng/ml 125nmol/L or more, together with early treatments (see the other articles here at Nutrition Matters), almost everyone hopes for an end to the pandemic, and do a return to normal, through some mix of the following:
One or more variants which are highly transmissible but relatively, or entirely, benign. These would be like a free vaccine, and they could run around humanity as our immunity wanes and top it up - continually suppressing the transmission of these variants AND the variants which cause serious disease.
Vaccines somehow being developed which provide lasting, robust immunity. (No such vaccines have ever been developed for coronavirus infections in any mammal.)
Theoretically, the first could be generated by genetic engineering, but there would be no profit in it compared to vaccines, so this will probably never be attempted.
The concept of a virus improving its fitness by reducing symptoms only applies directly to the symptoms which occur during the infectious phase of the disease. Generally, viral replication is not affected by the host being harmed or killed after this except to the extent that humanity gangs up on the virus and attempts to stop its transmission with vaccines, lockdowns etc. - or ideally with better nutrition and early treatment. Even then, the improvement in transmission is only to the extent that the host behaviour is no longer altered by the symptoms in a way which reduces transmission. (Some symptoms, like increased nasal mucous production or sneezing and coughing by people who don’t feel so sick as to avoid contact with others, increases transmission.)
These potential transmission gains are slim pickings with SARS-CoV-2 compared to the enormous scope the virus has for evolving generally higher performance in how it infects cells - so a single inhaled virus particle has a much higher chance of replicating. Early in 2021, Jiri Zahradnik and colleagues published a (preprint) article (link and my notes here) which describes how they used an elaborate, yeast-based (not using viruses) guided evolutionary experiment, to evolve receptor binding domain parts of the SARS-CoV-2 spike protein with greater and greater affinities for the ACE-2 receptor than any variant known at that time. This affinity is the electrostatic force which attracts and holds the spike protein to the protruding tip of the ACE-2 receptor, and so increases the chance of the virus infecting the cell in the presence of thermal vibrations and (I guess) other forces which would dislodge it before the fusion process takes place.
They independently evolved mutations which were found in known variants, and they evolved one set of mutations which produced about 640 times the affinity force of the original Wuhan variant. The British, “Kent”, variant of that time achieved its success due to having 3.5 times the affinity of the original Wuhan strain.
This is sobering research to contemplate. Firstly because it shows that Nature can make SARS-CoV-2 viruses evolve, on their own, to be much more transmissible, and likely to cause symptoms, as the variants to date. Secondly, because the article contains details of at least some of these mutations, and anyone with an RNA synthesis machine could use a text editor to craft a genome with the mutations, feed this to the RNA machine, pop the RNA into some cells and so create a batch of the super-high performance viruses . . .
Back to the question of how slim the pickings are if a SARS-CoV-2 virus evolves to have fewer symptoms: Hu et al. 2021-03-21, in pre-Delta Hunan, China, surveyed transmissibility and symptoms: www.nature.com/articles/s41467-021-21710-6. They reported:
The mean generation time was estimated to be 5.7 days, with infectiousness peaking 1.8 days before symptom onset, with 95% of transmission events occurring between 8.8 days before and 9.5 days after symptom onset. Most transmission events occurred during the pre-symptomatic phase (59.2%). SARS-CoV-2 susceptibility to infection increases with age, while transmissibility is not significantly different between age groups and between symptomatic and asymptomatic individuals.
So if we took whatever variant this was and made a second variant with no symptoms, its transmissibility would be marginally increased since without symptoms, presumably there would be unchanged social behavior and so more chance for transmission to new hosts. Since many people, in the Hunan context, are transmitting the virus even with symptoms, it seems unlikely that removing the symptoms would greatly increase overall transmission.
Quantifying Omicron’s immune escape
The three graphs at the start of this article are from a 2021-12-02 preprint reporting remarkable research and analysis of South African COVID-19 infections:
Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa
Juliet R.C. Pulliam et al.
www.medrxiv.org/content/10.1101/2021.11.11.21266068v2
Here is a short, qualitative, explanation. The steep rise in re-infections at the right end of the bottom graph is so high in proportion to the height of the primary infections (a person being infected for the first time) at the right end of the top graph, in comparison to these numbers during the Delta wave a few months ago, that we can conclude, just with our eyes and minds, that Omicron (which is causing most or almost all of the late November, very rapidly rising, infection wave) is causing a much greater proportion of its infections in people who were previously infected by Delta and earlier variants, than was the case for Delta or the earlier variants.
From this graph, I estimated that at the peak of the Delta wave, 1.7% of infections were re-infections, presumably of people who had been infected with earlier variants at least a few months earlier. In these very early days of the Omicron wave (the last data was for 27th November), I estimated that about 16% of the infections were re-infections.
South Africa’s relatively low rate of vaccination surely affected the transmission of both variants, but while these rates have been rising, the immunity it induced in earlier recipients has been waning, so the effects of the vaccination program probably haven’t changed a lot between early June and late November.
This apparent 16 / 1.7, Omicron / Delta, ratio of re-infection (and so escape from infection acquired immunity by prior variants in the months to a year or so before) is a dramatic change in how the virus infects a population of people. However, the actual change in viral behavior is somewhat less than this, since, as shown in the middle graph, the percentage of the population who could have been infected in the middle of the Delta wave was about 16%, and this has grown to about 24% by mid- to late-November when the Omicron wave began. Even then, combining these four rough figures, we find a very significant increase in the probability that Omicron will infect someone who has previously been infected: ((16 / 1.7) * (16 / 24)) = 6.3.
Immunity acquired from prior SARS-CoV-2 infection is widely thought to persist for years, but no-one can tell for sure yet how this would play out with the pre-Omicron variants regarding protection from infection or protection from severe symptoms (assuming the current parlous vitamin D deficiency persists, with no early treatments or even good vitamin D and other treatments in hospital). We can see from this beautiful research that this immunity against infection was never 100%, in this entire population of people (with all their nutritional deficiencies etc.) - and now we can see that Omicron really does escape such immunity much better than the previous variants.
I know of no data regarding Omicron escape from the narrower, weaker and more rapidly declining immunity which is induced by the current mRNA and adenovirus vector COVID-19 vaccines. I think it is reasonable to assume that Omicron will render these vaccines close to useless regarding infection - and so, to a large extent, transmission (though the immunity may still reduce viral shedding to some degree). However, I am an electronic technician and computer programmer and have no training or expertise in virology or epidemiology. Please make up your own minds about this and don’t quote me as if I am some kind of expert.
To what extent will Omicron escape the longer lasting ability of current mRNA and adenovirus vector vaccines to protect against serious disease? No-one can say for sure yet, but if - as seems likely - Omicron spreads very rapidly in northern hemisphere countries by the end of January, we will find out the hard way. The tragic way. The way chosen by those who guided the pandemic response to depend solely on highly profitable, slow-to-deploy, more harmful than advertised vaccines - which were made out to be far more effective than any coronavirus vaccine ever devised. (There there are coronavirus vaccines for cats - with the cats supposedly needing one injection every year.) The deadly way we will find out about Omicron transmission, immune escape and severity of symptoms is the way enforced on whole populations by the dismissal and suppression of nutritional repletion and early treatments which knowledgeable physicians and researchers have been desperately trying to raise awareness of.
Omicron causes hospitalisations just like prior variants
I am done preambling. (I learned this phrase from my wife Tina - she is the most accomplished preambler I know.) All the above is relevant to the question billions of people have been asking in the last week or so: Is this new, highly transmissible, variant likely to cause as much serious disease as Delta?
Assuming nothing is done regarding vitamin D, early treatment and better hospital treatment, then as far as I can see, the answer is YES. My opinion, as an electronic technician, counts for nothing. I am your guide to the observations and their interpretations. Here is what I think. You should decide for yourself what this means.
The 2021-12-03 figures from:
show that COVID-19 hospitalisations in South Africa have risen rapidly, from a very low base (compared to the peak of the Delta wave) in the last two weeks or so. The following graphs, taken directly from the above page (fullscreen the initial graph) show the rising numbers of daily hospital admissions in the top graph, and, in the bottom graph, the rise occurring primarily in Gauteng province which is where Omicron is most prevalent.

You should probably double click this so your browser expands the image.
So this means that in the Gauteng epicentre of Omicron transmission, the rise in hospital admissions is, very approximately (60.1 / 15.8) = 3.8 times as pronounced as it appears in the top graph.
I can think of no other explanation for these observations than that Omicron infection, in this population - protected only to some extent by prior infection and/or vaccination, with summer vitamin D levels which are better than in winter, but still terribly low compared to 50ng/ml, and generally lacking early treatment - affects people severely enough that quite a lot of them need hospital treatment.
The vaccine manufacturers are scrambling to make new versions which raise immunity to the Omicron spike protein structure. However, this will be of little use for reasons including:
It will take them months to get the vaccines into production.
Even if they are approved instantly (they should only be approved after years of testing) this will be too late for a large proportion of the population subject to low winter vitamin D levels. (See my seasonality article: nutritionmatters.substack.com/p/covid-19-seasonality-is-primarily.)
Even if hundreds of millions of vaccine doses could be produced now, it would take 3 to 6 months to administer them to most of the population.
By the time this is attempted, there’s a good chance that Omicron - being a much more raw, not yet subject to much evolution, virus than Delta - will evolve into multiple immunologically distinct variants of concern.
In other words, this currently “one” variant is likely to split into several, each competing to avoid the immunity generated by infection with prior variants, infection with other Omicron variants, and likewise by current and near-future Omicron-tuned vaccines.
If this happens, then Omicron will be known as the Death Star of the pandemic, until, perhaps, another even more destructive variant evolves. This is another reason to get our nutrition and early treatment houses in order ASAP - to reduce infections and so the chance of more proliferation of high-performance variants.
The current disastrous response to the pandemic is a man-made disaster which defies brief description. The quasi-religious fervor for, and faith in, vaccines plays a central role in its etiology, as reliance on this intervention is maximised, by suppressing discussion and knowledge of competing interventions, which actually are safe and effective, but not so attractive to governments and corporations due to being decentralised and unprofitable.
The pandemic was already going to get far worse with Delta and this northern winter, as the transmission protection of current vaccines waned, and as governments chased diminishing returns trying to vaccinate their entire populations with ever-increasing frequency, in large part to try to stave off declining protection against severe disease and death in the current, miserably inadequate nutritional and treatment circumstances. This nightmare is already developing rapidly.
According to what I now believe about Omicron, it is going to be very much worse.
The pandemic can only be suppressed by robust vitamin D supplementation and early treatment. This will greatly reduce the number of people who need hospital treatment - partly by improving the outcome for each infected person, but mainly by reducing disease severity, and so viral shedding, and so overall transmission.
These are all inexpensive, well-researched, broad, safe, effective ways of suppressing the pandemic - which the virus can't escape by altering a few amino acids in a protein.
Humanity will eventually discover this. I am just trying to bring that day forward.
Please help by spreading the word, including especially by encouraging medical professionals, immunologists, virologists, epidemiologists and public health administrators to read the research articles cited at:
What every MD, immunologist, virologist and epidemiologist should know about vitamin D and the immune system
vitamindstopscovid.info/05-mds/
The conventional pandemic suppression flowchart leads nowhere
The link at the start of this article was to a video by a comedy outfit.
The diagram below is no joke. It comes from Professor Freedom's Twitter perch:
twitter.com/prof_freedom/status/1433515417797005321
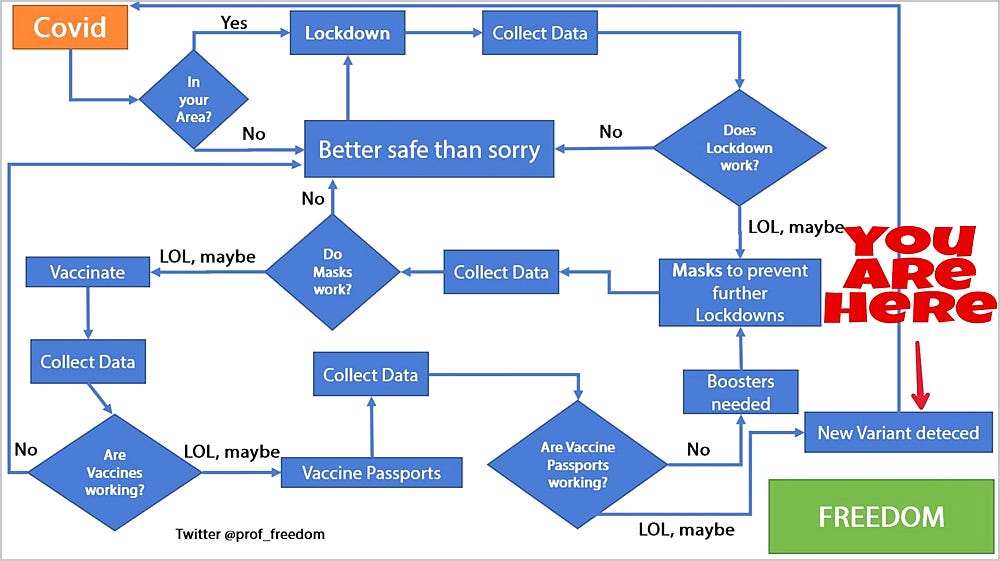
Individually, we can very largely protect ourselves from serious symptoms by supplementing vitamin D properly, and using early treatments.
However, freedom - remember those days? - will only return to whole countries once the great majority of people attain the 50ng/ml 25-hydroxyvitamin D levels their immune system needs to function properly AND have immediate (no appointments and trips to the pharmacy) access to early treatment. No-one can know for sure how well this will suppress Omicron or later variants, but it would be the height of lunacy to continue plugging away with vaccines, masks and lockdowns without fixing the gross nutritional deficits which render most of the population weak and prone to deadly inflammation, as they battle these increasingly nasty variants.
Please see the next article:
https://nutritionmatters.substack.com/p/omicron-rolling-updates
for updates on Omicron and related matters. I will add that article every day or two according to what transpires.
One of the links is to an article about a SARS-CoV-2 infection in an immunocompromised (HIV) person persisting for 7 months, and accumulating 30 mutations - I guess in multiple branches of genetic variation.
With 8.2 million HIV sufferers in its 60 million population, South Africa could be a place where the virus does this in an individual, and so acquires more mutations than would normally arise in normal replication from host to host. This is relevant to some of the discussions about history of the virus in general, and of Omicron specifically, at the Ethical Skeptic Twitter feed which Barry O'Kenyan referred to. Thanks Barry!
Big fan of Vitamin D for years! Keep my level at a steady 55-65. Are you defining the reinfections as symptomatic reinfections or just positive PCRs? Those numbers seem so high given the Qatar studies, etc. T cell repertoires of ORF1 and other non-structural proteins of SARS2 should abort COVID despite very different spike with Omicron. Just curious. Thank you!