
Omicron rolling updates - it seems to be less virulent than Delta etc.
Updated 7th January: The collision between a high-performance COVID-19 variant and disastrously low 25-hydroxyvitamin D levels exacerbated by the current Northern Hemisphere winter

This article contains multiple updates to my 2021-12-04 article:

Subscribers (free) receive the initial version of this update article by email. I will add to the web version as new information arrives, but this won’t generate fresh emails, so please check with the web version to keep up with the latest.
Here are the topics covered in the updates below:
U01 4th December
Phylogenic diagrams show both recent and ~May 2020 origins for Omicron. No consensus on its origins.
Using a narrow tool such as a vaccine in an attempt to stop a rapidly multiplying and mutating virus reminds me of Mickey Mouse’s The Sorcerer’s Apprentice difficulties in Disney’s 1940 Fantasia.
Wear a mask indoors, be vaccinated and be boosted.
“March of the vaccine dead” in Parma, northern Italy. See U04 too.
U02 5th December
New cases, hospitalisations and deaths in Gauteng province, South Africa, suggest not just very rapid Omicron transmission (no-one disputes this) but rapidly rising hospitalisations, which is presumably a measure of disease severity. See U03 for an alternative explanations.
Deutsche Welle (DW, German government) News interviews with experts on Omicron virulence.
Steve Kirsch has been unable to get fluvoxamine FDA approved as an early COVID-19 treatment.
The Guardian’s article shaming and denigrating the unvaccinated etc.
Synopsis of The Real Anthony Fauci.
Matter of fact report from Vietnam - children hospitalised by a bad batch of Pfizer COVID-19 vaccine.
Spanish committee: vaccine passports are ineffective and may increase transmission.
Wikipedia: Omicron reported in 42 countries.
U03 6th December
South African report: Omicron’s mild symptoms so far.
Two Twitter threads debating Omicron virulence.
My suggestion for how a bunch of mutations might increase overall transmission by improving viral performance in aerosol dispersion and so improve overall transmission despite the same mutations reducing the performance of the virus in infecting cells once it is in the body.
U04 9th December
Reports of generally mild Omicron infections in South Africa are not necessarily a guide to what will happen this winter in Northern Hemisphere countries.
The effectiveness of the neutralising antibodies produced by the Pfizer vaccine is found to be about 41 times less for the Omicron variant than for the original Wuhan variant - though this is not a true measure of the full immune response elicited by vaccination.
Two mutationally distinct lineages of Omicron variant are now recognised.
More details of the Parma anti-vaccine protests in which names and photos of dozens or hundreds of people are presented, because the protesters believe they have been killed by COVID-19 vaccinations.
Reports of sports people suffering heart problems, and of a rise of general heart problems in the UK being attributed to “pandemic stress”.
Bad batches of current COVID-19 vaccines may cause many more more adverse events than most other batches.
U05 14th December
Omicron is spreading rapidly - a doubling time of 3 days in Ontario.
The first death from, or with, Omicron is announced in the UK.
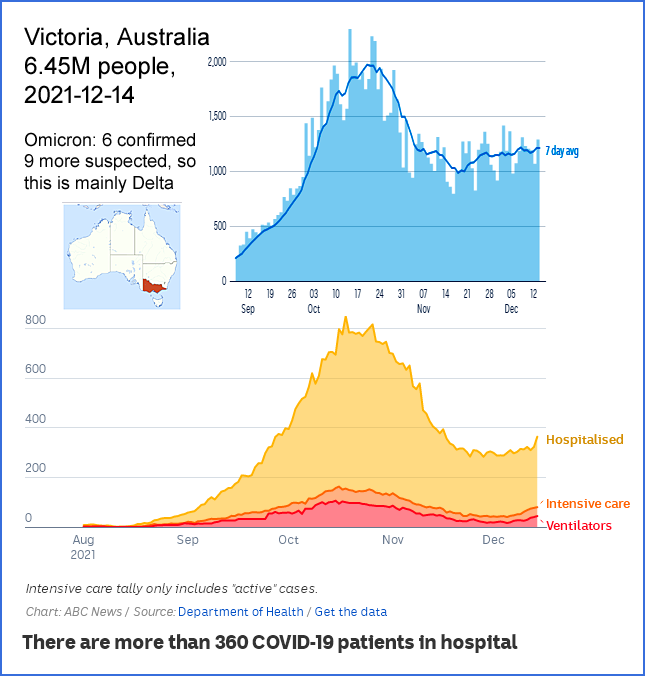
Victorian hospitalisation rates slowly rising, due primarily to Delta, so far - in early summer.
AstraZeneca vaccine deaths may be due to the adenovirus - not to its spike protein instructions encoded in its DNA.
U06 16th December
In vitro experiments indicate that Omicron reproduces less rapidly in the lungs than Delta.
Deaths from Delta rising steadily in northern European countries, entering winter.
U07 17th December
Video report from South Africa: “no evidence to date that Omicron is less severe than previous variants”.
U08 20th December
Two day doubling times and 7 deaths in the UK.
U09 23rd December
I see nothing conclusive yet about severity of Omicron vs. Delta in populations with low vitamin D and no access to early treatments. There are some indications of it being milder, but it is too early to tell, and there is no clear experiment since the natural and vaccine-acquired immunity status of populations has changes since the start of the Delta wave.
The difficulty of reconciling official reports of adverse reactions to mRNA and adenovirus vector COVID-19 vaccines with less academic sources of information about these.
U10 24th December
Encouraging signs from London that Omicron is less virulent.
U11 5th January 2022
Except for perhaps greater hospitalisations among children, all signs point to Omicron being less virulent than Delta or previous variants, even in low-vitamin D populations in the current Northern Hemisphere winter.
If most of us are infected with Omicron, why would we want to keep getting COVID-19 vaccines? There is no good reason, but the COVID-19 Vaccine Civil Wars are ramping up, so don’t expect the vaccinophiles to back down any time soon. French President Emmanuel Macron vowed to “piss off” the unvaccinated, who he described as the “worst enemies of democracy”.
Scott Davison, CEO of Indiana-based insurance company OneAmerica made some statements about excess deaths which some people are regarding as a sign of deaths caused by COVID-19 vaccines. See U12 too.
U12 7th January 2022
Pointers to an interesting discussion on the concerns about excess deaths, with alternative explanations and comparison with other countries.
Vaccine injuries are more common than generally believed - and some or many doctors and nurses are avoidant about what is going on.
Preamble . . .
How is there not going to be a global disaster in December 2021, leading into 2022?
The Omicron variant - with its unprecedented transmission speed - looks set to spread to all countries and infects tens or hundreds of millions of people, including some who have immunity from prior infection and many who have narrower, rapidly fading, immunity induced by mRNA or adenovirus vector vaccines. I expect this pre-existing immunity will protect against severe symptoms to some degree, but we don’t yet know to what extent.
This will be greatly exacerbated by generally lower than normal 25-hydroxyvitamin D levels in people of countries 25 degrees or more north of the equator - and for many or most people, normal is already a half or less of what immune systems need to function properly. I expect Australia and other southern countries such as South Africa will have a rough enough time with Omicron even as we enter summer - and it will be our turn for greater difficulties from May 2021 onwards as 25-hydroxyvitamin D levels drop again - unless we can raise awareness of vitamin D beforehand.
Since late March 2020 I have been trying to raise awareness of the need for robust vitamin D supplementation to support full immune system strength. I now collaborate with researchers and physicians - some are both - in this work, including New Jersey based retired Professor of Medicine, Sunil Wimalawansa (CV, keynote speech) who wrote his first article about vitamin D and the Wuhan coronavirus at the end of January 2020. It was published on 1st March, unfortunately in a predatory journal, which he chose in an effort to make the article available as soon as possible.
Twenty months later, while I know momentum for vitamin D awareness is building, I am profoundly frustrated by how difficult it is to get many physicians up to speed on this. There are numerous problems, including the frequently poor and misleading nature of some of the thousands of vitamin D journal articles which are published every year.
But spare a thought for Sunil and other professional researchers and physicians who have been on the case for decades! The most common response, he told me, was that “it couldn’t be true, it is just too simple”. The full, messy, details of the barriers we face in getting the majority of physicians to properly understand vitamin D will be the subject of future articles. We have to solve this. There is no workaround. Human health and happiness depends entirely on the medical profession getting crucial things right.
~ ~ ~ ~ ~
For me, the pace of change in this unfolding crisis picked up dramatically in early September 2021, with President Biden’s vaccine mandates, and with similar developments, lockdowns, protests, suppression of discussion of early treatments etc. which have accelerated since then in many countries.
My perception of the pace of change ramped up again on 2021-11-26 when the B.1.1.529 variant was known to be spreading with alarming rapidity in South Africa, and when its unprecedented number and variety of mutations was announced. That was 8 days ago. This was soon named Omicron and many people were hoping that it would not cause serious disease. Support for this optimism was given by early reports from doctors who reported no serious symptoms.
Yesterday (2021-12-03) I found the South African hospital data showing a rapid rise in admissions. That settled it for me - these hopes, which I never had any biological reason to believe - were false. So I wrote the article to which this one is an update.
Now - other than by a rapid adoption of vitamin D and early treatment - I can’t imagine how disaster can be averted.
I am reflecting on this, in the comparative calm, before what I fear will unfold. The speed of new developments is one aspect of this. At first I thought of two black holes, circling each other faster and faster - but that is rather grim. Instead, I think of my friend Valek Sadov, turning up the speed control on a Roland RE-201 Space Echo tape delay machine as he sang:
The world speeds up, you gotta speed up too!
before turning it down again for:
Living life in real-time’s hard to do.
That was in the early 1980s, in our Robin and Valek track, What a World - here mis-attributed to The Informatics.
Tina and I have some much more abstract music. You will need to bring your own imagination.
~ ~ ~ ~ ~
I believe we will put the pandemic behind us only when most people supplement with vitamin D properly, and the medical profession rescues itself from the drug company corrupted groupthink which afflicts most doctors today. That will be a profound revolution in health and happiness - something to fight earnestly for and look forward to. However, the enemy is not so clearly defined as in conventional war. The battleground is primarily in the minds of mainstream doctors.
Ideally we would all wake up tomorrow and this would be gone - or we would wake with a proper understanding of vitamin D and work assiduously to replete everyone we can, without coercion. That would be a new dawn for humanity - and most likely sunset for the pandemic. The beginnings of a well-informed, cooperative, supportive, public health program without fear can be found in the appointment of Dr Joseph Ladapo to the position of Surgeon General of the State of Florida. (Acceptance speech.)
We can’t know for sure that there will never be a variant - or some entirely new pathogen - which wreaks havoc on humanity even when we all have good nutrition, early treatment and plenty of 25-hydroxyvitamin D so our immune systems can work properly. But at least we will be better prepared.
One last thing: I oppose changing the rules regarding patents for COVID-19 vaccines, as has been suggested in the USA, to strip patent holders of their rights in order to allow anyone to copy their technology without payment. Firstly because vaccines are not the solution to this pandemic and secondly because there will probably be a time in the future when humanity seriously depends on vaccines, or other difficult-to-develop pharmaceuticals. We will have a much better chance of these being developed, with private sector innovation and vigour, if the commercial rules regarding patents are robust and not subject to arbitrary revision by unprincipled and desperate governments.
Here is the first update. The titles won’t cover every item they contain.
U01 2021-12-04: A much shorter phylogenic branch for Omicron?
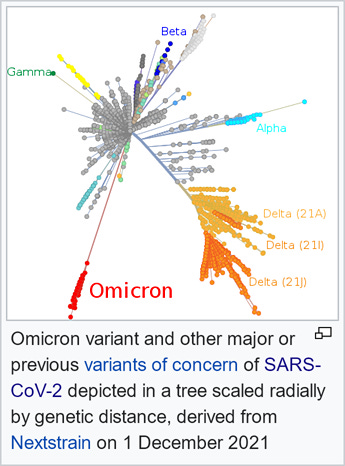
In the original article, the second graphic is a “A long new branch” image from Science Magazine, created in some way from nextstrain.org/ncov/gisaid/global . That depicted Omicrons phylogenic [WP] origins around March 2020, which is difficult to explain. But that was just for mutations in the S1 (outer) section of the spike protein.
The Wikipedia page shows a radial diagram with a similarly long branch back to what we assume is the early history of SARS-CoV-2, since genetic distance (number of changes) is generally assumed to correlate with how long such mutations took to evolve:
However, a completely different branch length and structure is shown at: nextstrain.org/ncov/gisaid/global?l=scatter
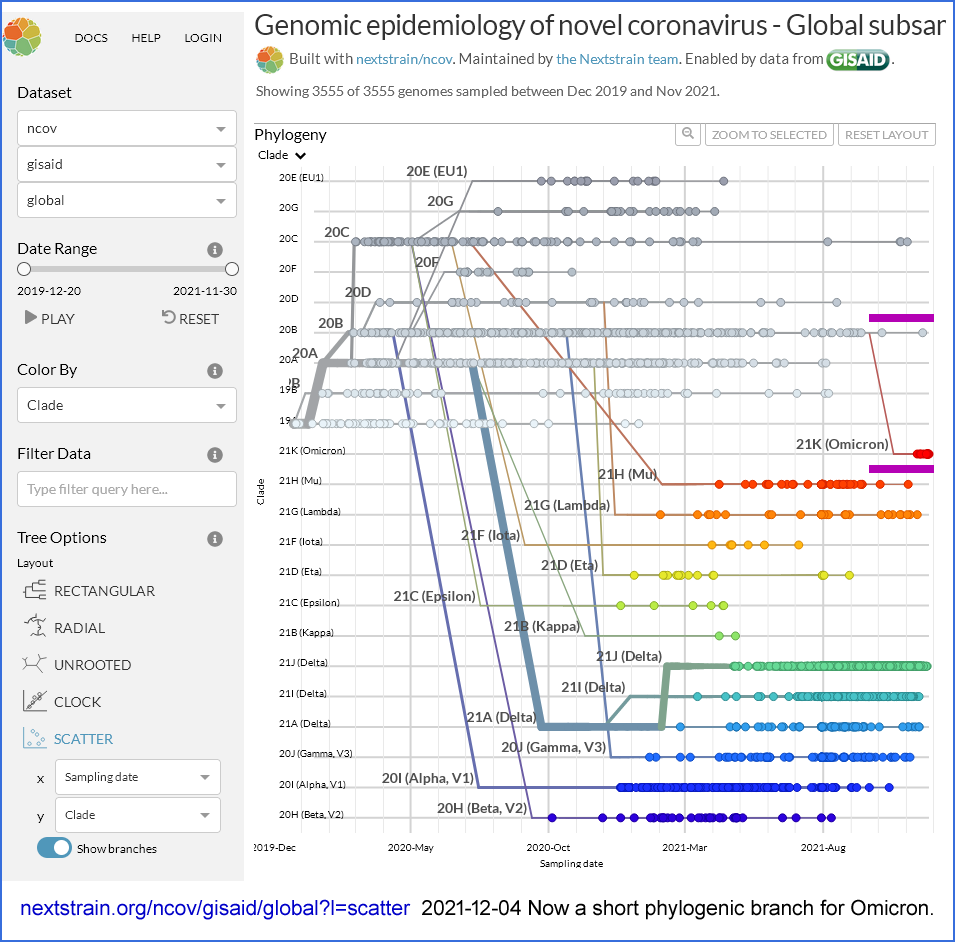
These diagrams are far beyond my understanding. In some respects, it doesn’t matter how the Omicron variant arose. In other ways it does, because it is always important to know the enemy and this is a rapidly changing threat environment.
Furthermore, our own actions, such as widespread vaccination programs and allowing the virus to persist for months in immunosuppressed individuals surely affects the evolutionary pressures under which a vast number of genetic changes emerge.
HIV-infected people have weakened immune systems, which can lead the SARS-CoV-2 virus to persist for months, splitting into numerous genetically different branches with large numbers of mutations. People suffering from autoimmune conditions are frequently given anti-inflammatory drugs, which also suppress innate and adaptive immune responses. It would be much better to start with substantial vitamin D3 supplementation, probably at higher than normal levels: vitamindstopscovid.info/06-adv/ . This would greatly reduce the chance of lingering SARS-CoV-2 infections.
The average mutation, if it has any effect on the structure of viral programs, is most likely to lead to a less functional virus. However, these can survive in an immunodeficient host, since they are already in an environment where there are new cells to infect. In theory, most of these mutated versions would not do well in the outside world, where they must persist in aerosols or on surfaces (fomites) and somehow enter another hosts’ body, find a cell with ACE-2 receptor, and enter that cell, while being subject to the destructive efforts of the host’s immune system.
According to Bloomberg there are 8.2 million HIV-infected people in South Africa (pop. 60M). One researcher reported that over a 7 month persistent infection, SARS-CoV-2 accumulated 30 mutations. It could not be ruled out that such heavily mutated viruses are viable, or even competitive with currently dominant strains. The extraordinarily sharp rise in prevalence of Omicron proves that this can happen, even if we are never able to reliably ascertain its origins.
For their own sake HIV sufferers should have their 25-hydroxyvitamin D levels lifted to at least 50ng/ml. A Google Scholar search for HIV "vitamin D" indicates such people would benefit from proper 25-hydroxyvitamin D levels anyway, and this, with multiple early treatments, would probably rid many of them of lingering SARS-CoV-2 infections.
In the 1960s, we all watched Disneyland on Sunday night and so were fully aware of the dangers of messing with uncontrolled, potentially, replicative systems - as in the case of Mickey Mouse’s botched attempt at thwarting his unwise creation:

The best free video of this part of The Sorcerer’s Apprentice I could find is of poor quality. This is from Walt Disney’s 1940 Fantasia - and I fear that with the passing of time, such lessons from history are not being learned by younger generations. Once seen, they could hardly be forgotten.
Lingering infections with rapidly mutating coronaviruses, pressure from leaky vaccines to evolve protein structures which escape current immune responses . . . what could go wrong?
~ ~ ~ ~ ~
13 cases of Omicron are known in the Australian state of New South Wales, mainly from local transmission or infection during flights to Australia.
The UK has 134 known cases of Omicron, half of them in people who, to use the coarse language of the day, “were double jabbed”.
Germany is excluding the unvaccinated from all but “essential” shops, as has been the case for a few weeks here in Victoria, Australia. The German government is also contemplating mandatory vaccination, as Austria is imposing. I am not sure to what extent these countries accept infection-acquired immunity as an alternative to vaccination. This is not an option in Victoria. All Victorians who work outside or in contact with others have had to be vaccinated.
The UK government wants every vaccinated person (currently two injections) to get a booster three months after their second injection, starting with those over 40 but extending to 18 year olds and over. Even the government refers to the injections as “jabs”. The minister refers to a “booster program” on steroids and states: “This is a national mission and we all have a role to play – so step up, roll up your sleeves, and get protected when the time comes.”
President Biden announced “All adults should get a booster shot six months after they got vaccinated (or two months after, if you were vaccinated with Johnson & Johnson). . . . We must vaccinate the world . . . ”.
Dr Gregory Poland of the Mayo Clinic is adamant in his advice on protecting against Omicron: “Wear a mask indoors, be vaccinated and be boosted.”
I found no evidence of officials in any country contemplating responses to Omicron other than vaccination, despite the plans of vaccine manufacturers to create Omicron-specific vaccines, due to the expected inadequacy of those currently in use - with such products surely taking many months to become available.
There are multiple reports of a March of the Vaccine Dead, in Parma, Italy - but perhaps they are derivative of a single report. Can anyone fluent in Italian confirm that the announcement of apparently dead people’s names in the video at that page is consistent with this march being as described? (See U04 below for one such response.) In the current environment of suppression of information which is critical of the pro-vaccine official agenda, it would not surprise me if such things did occur and were not mentioned at all by mainstream news organisations. This is a very large number of people who have apparently been killed - but the marchers could have traveled from afar.

See U04 below for further research in this and other protests in Italy.
The subject of harm and death from the current mRNA and adenovirus vector vaccines, to the extent that this is beyond what is officially acknowledged, is a huge topic which requires very careful scrutiny. I have not had the time to do a proper job of this, but I see a lot of worrisome evidence. Here is one such item: a report on a 2021-11-29 UK government clinical guidance document on myocarditis and pericarditis after COVID-19 vaccination.
U02 2021-12-05: Deaths rising in Gauteng province, South Africa
South Africa’s most populous (15.8M of 60.1M) and most densely populated province is the epicentre of the global Omicron COVID-19 wave. Many people all over the world hope that the new variant - which is obviously much more transmissible than any prior variant - will not lead to as serious disease as Delta or previous variants.
They have been encouraged in this by some South African doctors who reported no Omicron-related hospitalisations to date, the W.H.O. apparently stating that no Omicron-related deaths had been reported, by the general theory that viruses evolve to be less virulent and by a report by a French professor who calculated that Omicron was less transmissible than Delta. Please see my previous article on these nutritionmatters.substack.com/p/omicron-causes-hospitalisation-like to which this article is a rolling update.
Some of these people consider alarm about Omicron to be unjustified, and perhaps a ruse to boost vaccination sales and government encroachment on freedoms. However, as far as I can see, all the emerging evidence points to Omicron being, very approximately, as virulent as Delta - and much more transmissible.
See U04 for an update on these graphs three days later.
This page: gpcoronavirus.co.za/#cases/province.GP/Cases provides the latest data for Gauteng. The “Cases” box at the top left enables us to see deaths and hospitalisations. Here are the most recent graphs, showing the entire of the Delta wave, and the beginnings of the much more sharply rising Omicron wave. This is in South Africa’s summer with rising 25-hydroxyvitamin D levels, which surely played an important role in the last few months of decline of Delta cases) along with the most vulnerable people acquiring natural immunity or being killed by it - and by vaccinations, which began in May and are now numbered (I assume injections rather than people with 2 doses) at about 7.2 million. I guess this means about 4M of the 15.8M people have had two doses.
In the midst of this, cases and hospitalisations are rising at an unprecedented rate, and deaths are rising slowly, as one would expect with a lag of 3 or more weeks from infection, for a virus which does indeed cause serious disease:
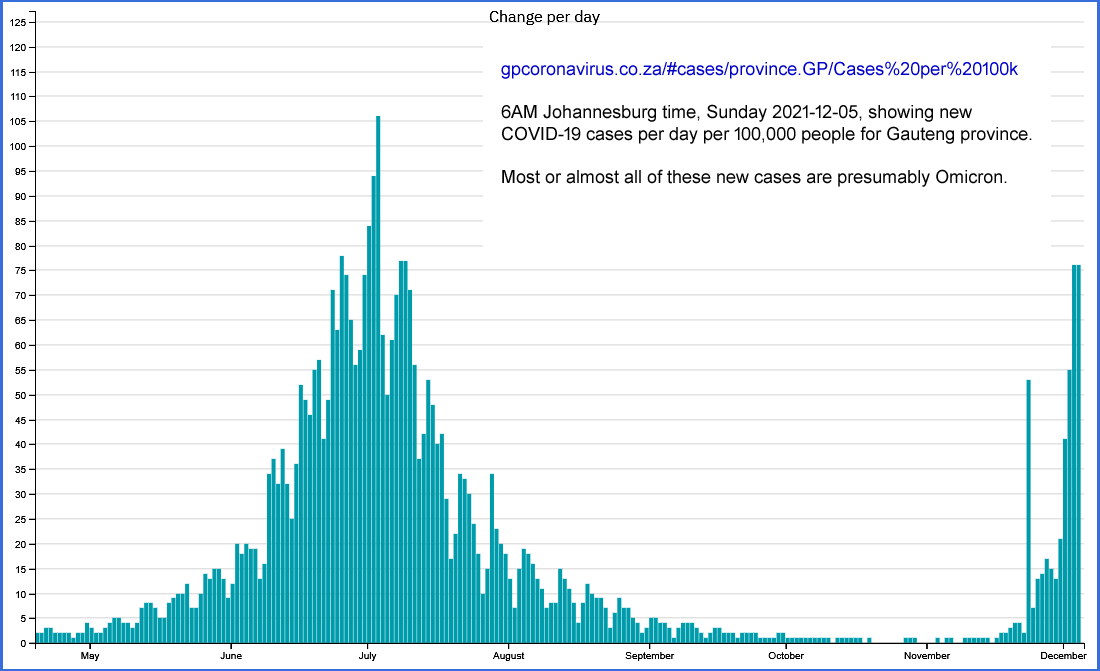
This was 6AM Sunday, Johannesburg time. I would expect a more complete update of figures by Monday evening, or by Tuesday sometime, to include the results of tests sampled and processed on Monday after a presumed drop in new test results over the weekend. This rate of rise is very approximately 5 times as fast as with Delta, or the two previous waves (not shown). Because of the publicity, the number of people tested may have risen somewhat, but this is still a very rapid rise in PCR detected cases. If the trend continues, this will indicate that one person per thousand, of all ages, in Gauteng is contracting Omicron.

I am not sure what the mid-November reduction in hospitalisation means, but it is clear that hospitalisations have been rising significantly with about the 1 week or so delay after PCR positive case confirmation. The rate of hospitalisation seems to be roughly the same as in the lead-up to the peak of the Delta wave, as is so for the new cases.
On this basis, our eye and mind can easily discern that Omicron is not very greatly more or less likely to cause serious disease, since hypoxia - which is what brings most people to hospital - is the first sign of the severe COVID-19 due to the immune system’s overly inflammatory response to the viral infection in the lungs. That infection itself may also cause some of the ill-health - but by whatever definition, lung infection, fluid in the lungs, destruction of the endothelial cells there (which line the blood vessels) etc. constitutes severe disease.
Most people - including doctors and nurses - have no idea that if the person had good 25-hydroxyvitamin D levels and/or (preferably AND) multiple early treatments, they would never get this sick - and that once they need hospitalisation, these treatments, with calcifediol to boost 25-hydroxyvitamin D levels safely over 50ng/ml in 4 hours, would enable most of these people to recover rapidly. These healthcare professionals should read the research articles I cite at: What every MD, immunologist, virologist and epidemiologist should know about vitamin D and the immune system: vitamindstopscovid.info/05-mds/
Since deaths due to COVID-19 infections lag 3 weeks to several months after initial infection, and since PCR diagnosis of infections (and so the case count) probably lag a week or so after infection, we would expect to see some rise in deaths as a result of the Omicron wave, if - as we fear - Omicron is not very much less virulent than Delta.
This is exactly what I percieve in Gauteng province. Again, Tuesdays figures would tell us more than these, but I think the trend is clearly upwards:

While Omicron may well evolve into several variants with potentially different disease-causing characteristics, and one or more of these might be less virulent, I see no reason to expect this to happen, except by good fortune.
~ ~ ~ ~ ~
D W News (Deutsche Welle) reports:
More young children are being hospitalized, and authorities are concerned that people who've already had COVID-19 are being reinfected.
Professor Wolfgang Preiser, Head of the Division of Medical Virology, Stellenbosch University, South Africa said:
We are also now experiencing such a rapid surge in case numbers that it is quite frightening.
I am moderately confident that the country will be able to cope. On the other hand, the rapidly increasing numbers are a nasty surprise - and I wonder what the future holds for us.
We are seeing a lot of breakthrough infections in vaccinees, which is, of course, a worry.
We are also seeing re-infections in people who have previously been infected during one of the previous waves. The majority of infections so far are mild.
That said, it is still early days. To become clinically severe there will have to be 10 to 14 days or more after becoming infected. So it is probably too early to tell.
German molecular biologist Kai Kuperschmidt, who wrote the great Science article mentioned in my previous article, said:
Those first puzzle pieces add to the concern - (re-infection) - and it does seem to be spreading very fast, though this is very hard to tell in the early days. . . .
He said there hadn’t been any deaths from Omicron in South Africa, but he said it takes two weeks from the time that people go to the hospital for death to be reported. He said we all want to think this is a mild variant, but that we should not pin our hopes on this.
~ ~ ~ ~ ~
Here are some recent developments broadly concerning the safety and efficacy of the mRNA and adenovirus vector COVID-19 so-called vaccines. These are not vaccines by prior definitions, but there is no other practical way to refer to them now. The question of vaccine safety is vast and contentious. I see far too many worrisome things to believe that public health officials and the mainstream, left-woke dominated, media is giving the public the full picture.
~ ~ ~ ~ ~
Steve Kirsch writes about his inability to get the widely used SSRI (Selective Serotonin Re-uptake Inhibitor) drug fluvoxamine approved for treating COVID-19, after he has spent millions of dollars in the last year or so proving, beyond any reasonable doubt, with RCTs, that it is safe and effective:

Basically, the system is set up so that only proprietary drugs that can kill you are approved.
So I wasted a lot of time and millions of dollars on proving that fluvoxamine works against COVID. I was right it does work. But Fauci is only going to allow a big Pharma solution to be adopted. Doctors do not follow the science. They follow what the NIH says. I should have known better. All these scientists had promised me “once it is proven in Phase 3 trials, everyone will adopt it.” That was a big fat lie. I fell for it. I won’t be so naïve the next time.
Note: I didn’t used to be so cynical, but there is simply no other rational explanation for this. This isn’t about science. This isn’t about saving lives. This is about profits and big pharma. Get it? I finally did. It was an expensive lesson.
Fluvoxamine is a prescription drug which may achieve its antidepressant effects, in part at least, by reducing inflammation in the hippocampus [WP], where we need a continual process of neurogenesis [WP] to not be depressed. Its anti-inflammatory properties apparently help reduce COVID-19 severe symptoms. Fluvoxamine is one of many COVID-19 early treatments analysed at: c19early.com.
~ ~ ~ ~ ~
Here is an outstanding example of the now well-established tradition of shaming, denigrating and ostracising the unvaccinated - while trying to scare them into compliance with mainstream medical advice to accept the injections, currently two, but with a booster within months:
If I’d known, I would have got it: on the frontline of Australia’s ‘pandemic of the unvaccinated’
Overworked doctors and nurses are digging deep to find compassion for patients who chose not to have a Covid vaccine
Cait Kelly and Tory Shepherd
The Guardian 2021-12-04
An unvaccinated patient lies on a hospital bed. Sick, dying of Covid, realising too late they should have got the jab.
Another, ill and panicking, asks if they can get the vaccination now. It’s too late, the doctor has to tell them.
Yet another, gasping for air, can’t even find the breath to ask.
This is what Australia’s doctors and nurses are dealing with, on the frontline of the “pandemic of the unvaccinated”. People realising the severity of their error, the outcomes of believing the misinformation that has been spread about vaccines, and the existence of Covid itself.
While it is really stupid to doubt the existence of COVID-19, or think about 5G cellphone tower radio waves and Bill Gate’s microchips, there is much more to opposition to the current vaccines than this article depicts.
This stinker is full of condescension, manipulation etc. However, I think the authors deserve recognition for this pungent new triplet:
But in that cohort, there is a firmly belligerent rump. Thousands of people have attended so-called “freedom” rallies, protesting a grab bag of Covid issues.
Belligerent threatening of politicians and healthcare workers is not OK, but Guardian vaccinophile people are likely to regard stalwart defense of scientific debate and personal autonomy as belligerent denial of facts and social responsibilities.
~ ~ ~ ~ ~
Robert F. Kennedy’s book The Real Anthony Fauci is 7 and going down on the NYT non-fiction best sellers list but is number 2 in books (not just non-fiction) at Amazon. Despite being released only 20 days ago, it is number 32 in books for the whole year. Written by a lawyer, the book presumably doesn’t contain much in the way of actionably false, defamatory material. 96% of the reviews are 5 star.
Chris Masterjohn PhD. provides a synopsis which itself looks tiring to read. He wrote, in part:
. . . this book is much more broadly about the global overthrow of constitutional democracy. Fauci and Gates get special naming in the title because they built what I will call the Global Pharma Machine. The climax of the book, however, covers the rise of the biosecurity state that hijacked this machine to turn it from a profiteering scheme into a final overthrow of constitutional governance . . .

Chris Masterjohn’s annotated copy.
~ ~ ~ ~ ~
A very substantial (20 years old, 241 journalists [WP]) Vietnamese online newspaper VnExpress reports, in a matter-of-fact manner: e.vnexpress.net/news/news/120-children-hospitalized-province-suspends-pfizer-vaccine-batch-4397748.html that an apparently bad batch of Pfizer COVID-19 vaccine put over 120 children, aged 15 to 17, in hospital, “after exhibiting symptoms like nausea, high fever or breathing difficulties”. The suspended batch is in storage to be used on adults.
Over the past week, three children have died following their vaccination with the Pfizer Covid-19 vaccine in Bac Giang, Hanoi and Binh Phuoc. The cause of death has been determined as "overreaction to the vaccine."
Last week, four workers in Thanh Hoa's Kim Viet Shoe factory died following their Vero Cell Covid-19 vaccination, also due to "overreaction."
~ ~ ~ ~ ~
The Telegraph reports that:
Experts from Spain’s inter-regional Covid committee have concluded that Covid [vaccination] passports are ineffective in terms of reducing infection, and may even be sending out the dangerous message that being vaccinated means a person cannot spread the virus.
~ ~ ~ ~ ~
Wikipedia en.wikipedia.org/wiki/SARS-CoV-2_Omicron_variant#Reported_cases reports 786 Omicron cases in 42 countries:

Three days later, the URL is en.wikipedia.org/wiki/SARS-CoV-2_Omicron_variant#Statistics with 1636 confirmed cases in 54 countries, and a total of 57,002 suspected cases reported from 10 of these countries. See U04 below about “stealth Omicron” not being detectable via PCR tests.
U03 2021-12-06: Arguments and perhaps evidence for milder Omicron symptoms
Here are some items I have not had time to evaluate. Perhaps there were younger patients in hospital at first. Perhaps some or many of those counted in the hospitalisation numbers were already in hospital for other reasons, and might not be all that ill, at least now. Perhaps reports of mild symptoms have been encouraged since many in South Africa are upset at travel bans imposed by many other countries when they think that nothing particular bad is happening, at least compared to what people overseas are fearing.
I only glanced at these and have no informed opinion yet:
www.samrc.ac.za/news/tshwane-district-omicron-variant-patient-profile-early-features A hospital in Pretoria, in the Tshwane district, gives details of cases to 2021-12-02. See U04 below for my thoughts on this.
John Burn-Murdoch seems to have access to quite a lot of data and can analyse it and make informative graphs. Some of his graphs appear in the Financial Times. See U04 for my thoughts - I don’t think he added anything significant to what can be learned from the hospital report.
 Okay folks, time for a South Africa update, focused this time on severity of disease. First up, the report from hospitals in Tshwane (the district furthest along in Omicron wave) is essential reading, as is thread from @miamalan samrc.ac.za/news/tshwane-d…[Thread] JUST IN: 1. NEW #OmicronVariant data from the Steve Biko/Tshwane District Hospital Complex via @MRCza. Tshwane = where SA's Omicron outbreak started 1. Data = for the 1st 2 weeks of the outbreak (14-29 Nov) 2. Past 5 days (29 Nov-3 Dec) = exponential increase in cases https://t.co/rbjpjEOQqQ
Okay folks, time for a South Africa update, focused this time on severity of disease. First up, the report from hospitals in Tshwane (the district furthest along in Omicron wave) is essential reading, as is thread from @miamalan samrc.ac.za/news/tshwane-d…[Thread] JUST IN: 1. NEW #OmicronVariant data from the Steve Biko/Tshwane District Hospital Complex via @MRCza. Tshwane = where SA's Omicron outbreak started 1. Data = for the 1st 2 weeks of the outbreak (14-29 Nov) 2. Past 5 days (29 Nov-3 Dec) = exponential increase in cases https://t.co/rbjpjEOQqQ Mia Malan @miamalan
Mia Malan @miamalanA related set of tweets: (Update - I didn’t find them very interesting.)


Here is my suggestion for how the virus could evolve to have both much greater transmission AND lower virulence:
Transmission involves viral performance, in all the circumstances, in a repetitive process which can be roughly broken down like this:
Virus is breathed in and lodges in the nose or throat. The viral performance of this stage is primarily determined by the probability that any one virus can infect a cell and so produce hundreds more. That may well start an infection.
A virus type which can do this with a 1 in 1000 chance of success is (all other things being equal) has a much higher performance than one which can do this on average 1 every 5000 times.Once the infection is established, performance is partly due to how well the viruses can escape destruction by the immune system. Part of this is how fast they can replicate.
In an established infection, how long can the host be made to produce viruses to be shed to infect others, and in what quantities?
To what extent can the virus alter host behaviour to increase the distribution of those viruses to other, so far uninfected, hosts? Making the host sneeze, cough, dribble etc. helps. Keeping them feeling good and sociable would help too - which might involve less symptoms.
Assuming, for simplicity, a purely airborne path of transmission, for every virus launched (in smaller droplets from breathing, speaking or singing, larger for sneezes and coughs), to what extent can the viruses survive all the journeys which might lead them to being breathed in?
There could be numerous factors at work here, including what happens to a very small droplet of water, and whatever else it contains, with a single virus. Does the virus dry out? If so, it cannot infect anyone. Can the drop shrink to a smaller drop than before, while the virus remains viable? If so, then this will remain aloft longer, and perhaps get through masks better.
It has been suggested that Omicron’s numerous mutations put a greater positive charge on the tips of the spike proteins. I have not tried to find the details, and I am sure it is a lot more complex than this description. Lets assume that this does happen: a large number of mutations greatly increases the viral performance in the aerosol droplet phase. So this is a boost, by a factor of 5 or 10, to the performance mentioned in item 5 above.
However, in this optimistic hypothesis, the mutations also reduce the performance of the virus in some or all of the other phases, or at least in phases 2, 3 and 4, in such a way that this reduced performance also causes less severe symptoms. Lets say this reduction in performance, and symptoms, is a factor of 2.
Overall, the virus still has higher transmission, but less symptoms.
Lets hope this is true!
Please remember that virtually all of the millions of people who are urgently discussing and trying to research Omicron’s virulence are clueless about the fact that almost all the people who are infected have very low vitamin D levels. Most of them don’t think about early treatment either.
If everyone had 50ng/ml or more 25-dihydroxyvitamin D and access to several early treatments, then very few people would need hospital treatment or die even if there were no vaccines, no infection-acquired immunity, no masks, no social distancing and no lockdowns. (Hand-washing and sanitation is always a good idea.)
So almost everyone is debating this as if harm and death, for any given set of host behaviors (which can be altered by lockdowns etc.) depends only on vaccine-induced immunity, infection-acquired immunity from previous variants and the raw transmissibility and virulence performance of the virus.
It doesn’t. We could suppress transmission and severity very strongly with proper use of vitamin D3, calcifediol for early treatment, and other early treatments.
U04 2021-12-08 The South African summer and potentially ivermectin assisted Omicron experience is not necessarily a guide to how Omicron will affect Northern European countries this winter
Three day later than when I wrote U02 above, 9PM Wednesday 8th December Johannesburg time, the Gauteng case numbers have not continued rising so fast, and may have fallen from the highest peak a few days ago. Deaths vary from day-to-day but are not noticeably lower. The hospitalisation graph at: pcoronavirus.co.za/#cases/province.GP/Hospitalisation (violet in U02 above) has not been updated, or at least records zero change to hospitalisations in recent days - so the graph appears as a left-shifted version of the copy above from Sunday 6AM. That last, bar, for Friday 3rd December, ~154 above, has been updated to exactly 160 now, but there is no bar at all for 4th, 5th , 6th or 7th December. We don’t expect one for 8th December, which is today.
Are they hiding the hospitalisation numbers? Do they think the numbers are unrepresentative of reality, or at least likely to be misinterpreted? If the numbers are in large part people who are in hospital for other reasons and happen to have returned a positive PCR test (as noted below), then this large number of hospitalised patients is not a alarming as if they were all admitted with hypoxia.
No other provinces show hospitalisation numbers in this system. Deaths are sporadic and not obviously falling in other provinces. Cases are clearly rising in all provinces since 25 November, but are not obviously rising since the peak around 4th December.
That peak might have been due in part to a peak in testing. PCR test numbers are not reported. See the note below on home testing leading to a reduction in government testing, so more people who test positive with home tests do not report that they are infected.
~ ~ ~ ~ ~
We should not necessarily assume that the South African experience of Omicron is a good guide to what will happen in other countries. It is summer there and Delta incidence was waning to very low levels - likely in large part to higher than yearly average 25-hydroxyvitamin D levels.
It seems to be routine in at least some South African medical practices and perhaps hospitals to use ivermectin to treat COVID-19, including as an early treatment - well before hospitalisation might be required. This would greatly reduce severity. This press release (undated, but searches reveal was from early February 2021) quotes Dr Angelique Coatzee as supporting the use of ivermectin for COVID-19 patients. She is the same senior doctor mentioned above, known around the world in the last week or so, who stated that in the cases she was familiar with, symptoms were mild. There was no mention of ivermectin in those statements. Nor was there any statement about how much better things would be if they could use it. So maybe an important factor in her patients and those of her colleagues was the use of ivermectin soon after PCR diagnosis.
Erik Starkman, whose blog covers many interesting health policy matters, noted on 2021-12-06 that NPR wrote on 2021-09-15 that many South African doctors do use ivermectin, but that they shouldn’t. The current government advice does not ban its use (following court cases which overturned previous bans) but goes out of its way to discourage its use.
~ ~ ~ ~ ~
I read the Tshwane (Pretoria - northern Gauteng) hospital report. The authors point out that this only concerns the first two weeks of patient history - and I guess that for many patients the time would be less than that. They write that it would be another 2 weeks before conclusions about severity could be reached with greater certainty.
On Thursday 2nd December (6 days ago) they report that 70% of their patients need no oxygen support. But these patients who do not need oxygen are not representative of normal COVID-19 patients admitted to hospital, because they note that:
These are the patients that we would call ‘incidental COVID admissions’, having had another medical or surgical reason for admission.
If this pattern, which is apparently novel and so did not occur in previous waves, is representative of the situation in general in South Africa in the last few weeks, then this indicates that the high hospitalisation numbers do not represent the same level of illness as in the past. This could be due to vitamin D, ivermectin, greater levels of vaccine-induced immunity, other seasonal factors affecting COVID-19 severity (vitamin D is the most important, I think: nutritionmatters.substack.com/p/covid-19-seasonality-is-primarily) AND/OR the currently dominant Omicron variant causing less severe disease. Another major factor, as the authors note, is that with the rapid rise in Omicron patients, hospitals have not yet had many such patients who were infected 3, 4 or more weeks ago.
Another factor is that at least 80% of these new patients were under 50 years of age.
A further factor not mentioned by the authors is that more people now have infection acquired immunity than the start of the Delta wave. (The increased level of vaccination would help too, but that immunity fades over months.)
This report summit.news/2021/12/07/healthcare-chief-says-omicron-may-signal-the-end-of-covid-19/ quotes Richard Friedland, the CEO of South Africa’s largest private health network, as stating:
If in the second and third wave we’d seen these levels of positivity to tests conducted, we would have seen very significant increases in hospital admissions and we’re not seeing that. In our primary care clinics it is mainly people under 30-years-old,” he said.
So I actually think there is a silver lining here and this may signal the end of Covid-19, with it attenuating itself to such an extent that it’s highly contagious, but doesn’t cause severe disease. That’s what happened with Spanish flu.
We are seeing breakthrough infections of people who have been vaccinated, but the infections we’re seeing are very mild to moderate. So for health care workers who have had boosters, it’s mostly mild. I think this whole thing has been so poorly communicated and so much panic generated.
But this is still South Africa, in summer. The test will be by the end of December, in northern hemisphere countries, where it is now reasonable to expect Omicron will largely displace Delta.
For whatever my completely untrained, unqualified, opinion is worth, I think these reports are consistent both with Omicron being equally virulent as Delta et al. and with it being significantly less virulent. It is early days and there are multiple other factors, including vitamin D and ivermectin, which are not reported or perhaps even thought about by the authors. Even if they don’t use ivermectin themselves, many South Africans individually, and via their doctors, may be doing so.
~ ~ ~ ~ ~
I read the Twitter threads mentioned above in U03. John Burn-Murdoch does not seem to have noticed that the 70% of patients in hospital not needing oxygen were those who were admitted for other reasons. He is apparently unaware of vitamin D seasonality or ivermectin use. At first glance I thought his analysis graphs might prove useful, but I think the don’t tell us anything different from what we have been fed officially.
I agree with his assessment:
So is Omicron inherently a more mild strain? No evidence either for or against that at this stage.
This image, from the Financial Times article of 2021-12-04 he contributed to, is instructive:
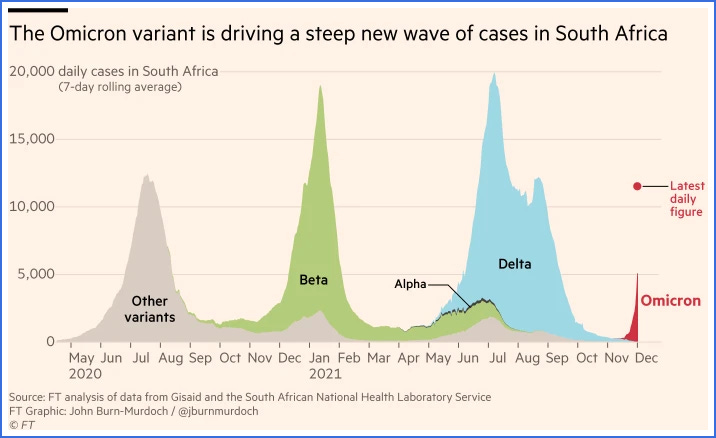
This is an alarmingly sharp rise in cases, going into summer.
~ ~ ~ ~ ~
This research article (not peer reviewed or even on a preprint server, though the file name mentioned medRxiv) looks significant:
SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer
BNT162b2 elicited neutralization and requires ACE2 for infection
Sandile Cole, ~32 others and Alex Sigal
PDF creation date 2021-12-08 6:34 (timezone?)
www.ahri.org/wp-content/uploads/2021/12/MEDRXIV-2021-267417v1-Sigal.pdf
Omicron exhibited a very high degree of immune escape to neutralising antibodies created by the Pfizer vaccine, using the blood from vaccinated subjects, some of whom had also been infected with prior variants, in in-vitro assays with genuine Omicron viruses (not created in the lab from a genome file) in cultured human cells.
Within hours of this being released an article appeared with comments by several scientists. The first (Jonathan Ball) put a positive spin on it by asserting that having two initial vaccine injections plus a booster injection would produce immunity comparable to those who had both the two vaccine and a natural infection. This is at odds with all we know about the narrow immunity elicited by mRNA and adenovirus vector vaccines and the broad, longer lasting, immunity which results in all parts of the immune system (including the nasal passages, not just the arm muscle) engaging fully with the entire virus in a genuine infection. That a virologist states this shows how distorted many experts’ thoughts, or at least statements, are by the need to support the vaccines to the exclusion of all official narrative.
The other three scientists said much the same thing. However, the last, Professor Penny Ward, cited two articles which she argues show that reduced levels of neutralising antibodies with prior variants does not make so much of a difference to vaccine efficiency: Lefevre et al. 2021-09-22 and Thomas et al. 2021-11-04 . Ideally I would scrutinise these, but I don’t have time to do so.
Back to the Cole-Sigal article: By diluting the serum from multiple subjects the researchers were able to estimate a dilution which resulted in a 50% inhibition of the ability of viruses to replicate in a supportive culture of human cells. The researchers first established that Omicron requires the ACE-2 receptor for cell entry, as expected (but there are discussions of it perhaps being able to us other receptors - and I have seen this suggested of prior variants). Secondly, they measured the ability of the mix of antibodies in the subjects’ serum to inhibit the replication of both the original D614G Wuhan virus and of the Omicron variant (bearing in mind that there are already multiple types of Omicron, as discussed next).
They found that the serum could be diluted to some concentration X to 50% inhibit the replication of the original Wuhan strain but that, on average, 41 times this concentration was required to similarly inhibit the Omicron variant. This is a very high degree of immune escape. However:
I don’t know a similar factor for Delta with the original Wuhan strain as a reference.
There is a great deal more to the full immune response than the direct actions of neutralizing antibodies [WP] which can latch onto an epitope (short, 3D, pattern of amino acids in part of a protein) and so prevent the virus from being infectious. (For instance, double-headed antibodies can bind two or more viruses together into larger, less mobile, assemblage in which no virus has a chance to properly align with an ACE-2 receptor.)
Neutralizing antibodies are important, and this confirms a high degree of immune escape by Omicron, at least to this aspect of vaccine-induced immunity.
All 12 subjects had received their vaccination (I assume the 2nd injection) between 10 and 33 days of the blood sample which was used in these tests. This is before any significant fading of immunity, and might be in a period in when immunity was still rising after vaccination. 6 subjects had not had prior infection and another 6 had been infected with D614G, on average just over a year before vaccination.
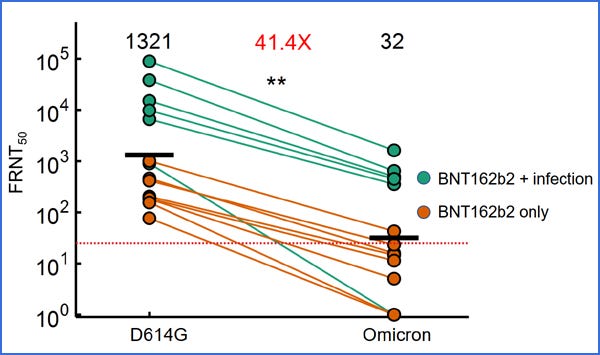
The vertical scale is logarithmic, with each step higher being a factor of 10 times greater dilution of the serum, and so of the antibodies it contains. Each pair of green dots, tied by lines, represents the serum of a subject who was infected by the early D614G variant about a year before being vaccinated with the Pfizer vaccine. The red dots represent the serum of the subjects who were vaccinated, but not previously infected.
We can see that those who were infected and vaccinated had much greater concentrations of neutralising antibodies in their blood, than those who were only vaccinated, since the serum from their blood could be diluted much more before it no longer achieved 50% reduction in viral replication.
We can also see that the Omicron variant was far less affected by these antibodies than the D614G variant since for each subject’s serum, Omicron required much less dilution of the serum in order that it could attain the 50% replication reduction, than was the case with D614G.
One of the 6 previously infected subjects had serum which provided weak neutralising antibodies, similar to the lower protection of those who were only vaccinated. The other 5 showed very much superior protection - and averaged greater protection (higher vertical position) due to the apparent strength of their antibodies (by their quality and their number) than the average protection attained by only vaccinated subjects for the original D614G variant. The worst outcomes (bottom right) - the weakest protection - as measured by how little dilution was possible before replication was no longer halved, were for Omicron with all the 6 just vaccinated subjects and with one of the 6 who had also been infected in the past.
This doesn’t tell us anything directly about risks of severe disease with Omicron - but we expect stronger viral replication to lead to more intense infection and a greater risk of developing lung infections, hypoxia and severe COVID-19. All these discussions are by people who have no idea that the immune systems of almost all the people they are treating, or studying, cannot work properly, due to having 1/2 to 1/10th of the 50ng/ml 25-hydroxyvitamin D they need.
In answering the question about to what degree vaccination alone, or vaccination and infection with prior variants, provides protection against infection with Omicron, or protection against severe outcomes, my answer is: Who cares? Get your 25-hydroxyvitamin D levels up to 50ng/ml or so ASAP and make sure you have access to several early treatments, in the event that you become infected. We probably will all be infected in the next few months, if Omicron’s rapid spread across the world is anything to go by. (I think that people with serious comorbidities probably should be vaccinated, even with good 25-hydroxyvitamin D levels and early treatments ready to go.
There is no data yet, but I think it is reasonable to assume that vaccination, with or without boosters, on its own - without prior infection, without proper 25-hydroxyvitamin D levels and without any early treatment - will provide only marginal protection against Omicron infection, and significantly less protection against severe symptoms than it does for Delta.
This research did not concern people who had solely infection-acquired immunity - it was only intended to quantify part of the capability of vaccination to reduce viral replication.
~ ~ ~ ~ ~
About a year after these mRNA and adenovirus vector vaccines were first deployed, we see that:
The muscle-based (not nasal passages, and so mucosal) immunity, they induce based solely on an already extinct design of the viral spike protein, is too narrow to reliably suppress the rapidly mutating SARS-CoV-2 variants.
Their protection against infection fades too fast to attain herd immunity - which was what everyone was promised a year ago, once 70% or so of the population had been vaccinated. Thanks to Alex Berenson, here is the FDA’s pitch in July 2022: www.fda.gov/news-events/fda-insight/fda-insight-vaccines-covid-19-part-1.
Their protection against severe symptoms (in all the disastrous circumstances of lousy 25-hydroxyvitamin D levels and no early treatment), while apparently longer lasting and genuinely useful with Delta, is surely going to be much weaker with Omicron and likely future variants.
They are slow to develop (months) in comparison to vitamin D and early treatments, which already exist.
They should take years to test, but even with compressed and incomplete testing they take months to test.
They take a few months to develop a new design for a new variant, not counting production ramp-up, testing and time to deploy - so they have a 6 to 12 month response delay, when we are dealing with a variant which can spread to 54 countries within a month of it first being identified.
They cost tens of billions of dollars for large fractions of the population, such as USD$20 or more per dose.
They are not as safe, or effective, as most people have been lead to believe.
So the current COVID-19 vaccines may of some use in protecting against serious illness - and the new, improved, versions will arrive too late.
A year from their introduction, reliance on COVID-19 vaccines alone has been shown most governments ‘ approach to the pandemic to be an unwinnable game of Whack-a-Mole.
The vaccineophile response has been to:
Urge everyone to get vaccinated.
Urge everyone to get their booster.
Bring forward the time after the second injection when boosters are available and required. So the status of being “fully vaccinated” is being redefined to require an increasingly frequent program of boosters.
Demonise the unvaccinated and lock them out of society and the economy in an effort to force compliance with unpopular vaccine mandates.
Urge the rapid development of boosters customised for the Omicron variant (but see below, this has already split into two major sets of lineages, with distinctly different mutations) and/or the creation of multivalent vaccines.
Multivalent vaccines have fundamental problems. To get good immunity to four designs of spike protein, all at the same time, would require four times the immune response. This may not be possible, but if it is, then it is likely to be undesirable since ill-effects scale with the stimulus which must be given to elicit such responses and/or with the intensity of the responses.
Alternatively, for a given level of immune response, the lasting immunity to each of the four types of virus will be weaker.
The vaccine juggernaut is still going strong - but this cannot last. Omicron is a turning point at which many people realise they have been lied to by experts they should be able to trust.
This means more people will take an interest in nutrition and early treatments.
~ ~ ~ ~ ~
While the world was in a tizzy about the Omicron variant’s immune escape leading to severe symptoms in those who have been only vaccinated (and who have poor nutrition and no access to early treatment) the heavily mutated, and very young, researchers split their model of Omicron into two lineages with distinctly different mutation patterns:

This is from ~2021-12-07: github.com/cov-lineages/pango-designation/issues/361.
The tree of diverging Omicron sub-types, in these early days, with most sub-types being classified in several Delta clades, is:

This is from: nextstrain.org/ncov/gisaid/global?branchLabel=emerging_lineage&l=radial&m=div&p=full&transmissions=show.
I haven’t yet read this new article on Omicron in Nature: www.nature.com/articles/d41586-021-03619-8.
~ ~ ~ ~ ~
People with access to home tests rarely report their COVID-19 infections to the authorities: www.statnews.com/2021/12/07/growing-use-of-home-covid19-tests-leaves-health-agencies-in-the-dark/
~ ~ ~ ~ ~
Regarding the “March of the Vaccine Dead” in Parma, northern Italy, a reader kindly informed me that his Italian wife saw the same or a similar video around the end of November. He wrote:
She said that it is (appears to be) people protesting the loss of friends or family to the vaccine. Names and ages are being read out. All ages in the clip she sent me (which I think is the same as the one you have posted ) are under 60.
Searching further with Duck Duck Go, I found this page with a video (click the arrow) of the same march which is clearly at the Pilotta Complex in Parma.
Another video of the march: www.bitchute.com/video/ascunl0yUzO8/ shows four people holding a sign TRIESTE CHIAMA PARMA RISPONDE:

TRIESTE CALLS PARMA RESPONDS
Searching Duck-Duck-Go for Trieste chiama turns up references to numerous protests against Italian government vaccine mandates, which were initiated in Trieste.
This was the Parma protest. The marchers were not protesting deaths due to COVID-19. I conclude that they sincerely believe that these friends and family were killed by COVID-19 vaccines.
I do not know how many of the people pictured in these marchers’ signs, who all apparently recently died, were in fact killed by COVID-19 vaccines.
It is unwise to completely dismiss earnest beliefs such as these without thorough investigation. The fact that so many people considered this to have happened, even if none of the deaths were caused by the vaccines, is a serious matter in itself. The government insists the vaccines are safe, and hundreds of people in these videos believe exactly the opposite.
~ ~ ~ ~ ~
Here are three items, some of many, which make me think that the problems caused by the current vaccines are not properly recognised:
An anonymous, but carefully written, analysis of deaths of footballers this year, and in previous years: dailyexpose.uk/2021/12/08/278-percent-increase-in-heart-attack-deaths-among-soccer-players/.
A video of recent heart attacks among sports professionals: www.bitchute.com/video/La3gSjtT6VBJ/.
The UK “explosion of new heart illnesses”, especially among younger people, is recognised by a vascular surgeon, who attributes this to “a direct result of the increased stress and anxiety levels caused from the effects of PPSD (post-pandemic stress disorder).”: summit.news/2021/12/08/explosion-in-new-heart-conditions-explained-as-post-pandemic-stress-disorder/
~ ~ ~ ~ ~
There is a series of investigations by an anonymous author at the dailyexpose.uk (which runs a plethora of stories, some of which I think are unreliable) which seem to be to be carefully done. This is the latest: dailyexpose.uk/2021/12/05/all-covid-vaccine-deaths-and-disabilities-in-children-caused-by-6-percent-of-batches/. It concerns the observation that the adverse reactions reported in the US VAERS database seem to be for only a small subset of the total set of reported batch numbers. I downloaded the VAERS .cvs files and manipulated some of the data sufficiently to ascertain that there was indeed a great imbalance in the distribution of adverse events vs. batch numbers. Assuming the batches all contain a reasonably similar number of doses, such as within a factor of 5 or 10, this is very difficult to explain except by the hypothesis that some batches really did cause a lot more adverse events.
This fits with the Vietnamese report mentioned above. Clearly not all COVID-19 school vaccination programs put 120 children in hospital - but this one did.
I could spend a week or two listing the most significant reports concerning COVID-19 vaccine reports - but my focus is on nutrition and early treatment. I can’t quantify what is happening regarding these adverse events, but I believe that the current mRNA and adenovirus vector COVID-19 vaccines cause a great deal more harm and death than the public is lead to believe.
This is an important part of how people respond to the increasingly forced nature of government COVID-19 vaccine programs. Some fears are irrational and others are based on real problems.
Even if these vaccines were as safe and effective as advertised - and perhaps the Novavax protein sub-unit vaccine will attain this goal - they would still be the third best approach to combating the pandemic after vitamin D repletion and other nutritional improvements plus multiple early treatments.
U05 2021-12-14 Omicron: First death in the UK; Doubling time in Ontario = 3 days
The Washington Post reports on 10th December that Omicron is spreading very rapidly in Europe:
. . . the omicron variant could become dominant in some countries startlingly soon, overtaking the delta variant . . .
“We expect it to overtake delta within days, not weeks,” Nicola Sturgeon, the first minister of Scotland, said Friday about the spread of omicron there.
[UK Health Security Agency estimate] it will become dominant in Britain by mid-December, with more than a million infections by the end of the month.
In Denmark, too, omicron on its current trajectory could become dominant by “the end of next week,” said Mads Albertsen, a professor at Aalborg University.
The suspected proportion of omicron among all coronavirus infections in Scotland surged from 2 percent Sunday to more than 15 percent Friday, suggesting that cases are doubling every two to three days.
CNN’s 13th December report mentions UK government statements:
UK Prime Minister Boris Johnson confirmed the country's first death of a person with the variant.
Health Secretary Sajid Javid said on Monday that there were 4,713 confirmed cases of Omicron in the UK, adding that the current number of daily infections is estimated to be around 200,000.
"While Omicron represents over 20% of cases in England, we've already seen it rise to over 44% in London and we expect it to become the dominant Covid-19 variant in the capital in the next 48 hours,"
"It's spreading at a phenomenal rate, something that we've never seen before -- it's doubling every two to three days in infections." He added that it was too soon to tell if cases of the new variant are milder.
"That means we're facing a tidal wave of infection, we're once again in a race between the vaccine and the virus," Javid added, echoing language used by Johnson in a televised address on Sunday night.
On Sunday, the Prime Minister set a new target of offering all adults a third shot by the end of December -- a month earlier than originally planned. He had previously cut the interval between second and third doses from six months to three.
"No-one should be in any doubt: There is a tidal wave of Omicron coming," Johnson said. "But the good news is that our scientists are confident that with a third dose -- a booster dose -- we can all bring our level of protection back up."
Javid said 10 people had been admitted to hospital with the new variant. The UK's Health Security Agency confirmed they were spread around the country and aged between 18 and 85, while the majority had received two vaccine doses.
~ ~ ~ ~ ~
The Australian Broadcasting Corporation reports today:
A [Newcastle, north of Sydney] public health controller is predicting a 70s-themed prom night at a Newcastle nightclub could become one of the highest COVID-19 transmission events in the world. . . . of the 650 people checked into the event, 150 people have so far tested positive to COVID-19, most likely with the new Omicron variant.
6 confirmed Omicron cases in Victoria, some locally transmitted, with sequencing underway for another 9 possible cases.
Vaccines for kids aged 5 to 11 start on January 10.
~ ~ ~ ~ ~
CBC News interviews Dr Peter Juni, Scientific Director, Ontario COVID-19 Science Advisory Table and Professor of Medicine and Epidemiology at the University of Ontario:
Asked about many people’s hopes that Omicron would lead to milder infections than those of previous variants, he said:
People are clutching at straws.
For a situation like South Africa, is is mile, most likely due to probably 93% of the population in Gauteng is immune either through infection or vaccination.
For people who have reached some immunity, it may be milder.
We don’t have any evidence to suggest that it will be milder.
In the roughly 20% of people in our province in Ontario who have not been infected or vaccinated, that’s the big challenge.
The interviewer mentioned that on the Ontario COVID-19 Dashboard he had given the Omicron R0 (reproduction number) as 3.32 - and that this number was followed by three exclamation marks. As I write this 2021-12-14 5:30AM UTC, the figure is 4.01, with no exclamation marks. Here, with my annotations in magenta:

This thing is roughly three times as transmissible as Delta.
The doubling time we see here is exactly compatible with what we see in the UK and everywhere else. We see it in Gauteng, we see it in the UK, we see it in Denmark.
This week we will [probably] reach 50% of all cases in Ontario being caused by Omicron.
At the time of the interview, the percentage of cases caused by Omicron was 21%. As I write this, it is 30.8%, above.
In Gauteng, it took 3 weeks for them to go from 5% to 95%. It is exactly the same here.
People are unable to imagine how fast this goes. We need to let go of the myth that this is mild.
[The increased transmissibility] is a combination of two things: One is intrinsic transmissibility - we don’t know by how much. The other part is that it evades the immune system.
Based on data from the UK, which he said was all consistent (implicitly with data from other countries) he said:
Those of us who are less than 3 months after the second [vaccine] dose still have quite a bit of protection.
We need to massively boost our 3rd dose roll-out. But that will not be to control the pandemic at the population level. [Muddled words about protection against hospital admission.] We just try to protect as many people as we can with the 3rd dose.
Remember, if you have had 2 doses, it will still be very protective against hospital admission, but its not 100% protective - so people really need to be careful now.
He mentioned that he was missing out on his 3rd booster dose because he was being interviewed. Where do we go with Omicron?
This is very challenging. We cannot control this with the vaccine. This will go too quickly.
If these numbers double every 2 to 3 days, this goes very fast.
So we need measures in place, immediately, to make sure that we are able to deliver it [the booster doses] and to make sure that we basically secure what is important: the hospitals, the long-term care homes and the retirement homes.
Loads of vaccines. Loads of rapid testing.
Its very simple. What works before works again.
These people are culpably clueless. They are paid good money to protect the population, but I as an electronic technician, and you as a reader of this and other websites, know more about how to protect everyone than they do.
They have no idea about the immune system’s need for 50ng/ml 25-hydroxyvitamin D.
We now decrease our contact rates. We see less people. We work from home.
Are water pipe repair crews (I reported a leak in our street at 4:30PM, a crew turned up within an hour and they fixed it and restored the supply by about 9PM), delivery drivers and interstate truck drivers going to work from home? What about doctors, nurses and paramedics? . . . . .
This doesn’t have to go back to where we were a year ago.
He is so calm and apparently oblivious to the manifest falsehood of his statements.
We need to dramatically act right now - because I agree with the people in the UK: it is a really massive wave coming.
Use good masks. Stop going into crowded places indoors.
Just stop it completely.
Let go of the myth it is mild. We don’t know about that - we will see what’s coming.
The picture of a tidal wave is correct.
~ ~ ~ ~ ~
Omicron arrived in China via a traveler from overseas, who is being quarantined. There is a Delta outbreak in the the eastern province of Zhejiang. Wikipedia reports that Omicron has been detected in 74 countries.
~ ~ ~ ~ ~
The ABC reports on Victorian case, hospitalisation, ICU and ventilated patients in ICU numbers rising slowly after the lockdown ended. Unvaccinated people are not allowed in most shops, cafes etc. - but there are no travel restrictions. Masks should be worn in public places. Considering we are going into summer, this is bad enough as it is with primarily Delta driving hospitalisation and cases so far.
It is reasonable to expect Omicron to make things much worse, but to what degree rising 25-hydroxyvitamin D levels, the effects of booster vaccinations and any new lockdowns will have against this is impossible to predict. I expect most of us will get Omicron in 2022.
Hopefully people will get out more, raising their 25-hydroxyvitamin D levels and this will suppress transmission and severity. The solar peak is the solstice - December 21. However, there are multiple reasons COVID-19 infection suppression lags considerably behind this, and for hospitalisations and deaths to lag further still:
The temperature of the upper layers of the ocean lag the solar radiation peak. This controls the air temperatures which peak in mid-February.
BTW, the Earth’s orbital eccentricity means we are about 3.3% closer to the Sun in the southern summer than in the northern summer, so the southern summer Sun radiant power per square metre is about 6.9% greater than in the northern summer. Fortunately, there is more ocean in the southern hemisphere to moderate what would otherwise be a greater temperature excursion.UV-B skin exposure depends partly on the UV-content of sunlight, which peaks with the solstice, but also to a large degree on the temperature which gets people out of the house with less protective clothing. So the UV-B exposure peak is probably late January to early February.
The D3 produced in the skin takes a few days to be hydroxylated in the liver to add to the circulating 25-hydroxyvitamin D which is the immune system needs. Depending on its level, its half-life of this 25-hydroxyvitamin D is weeks (high level) to two months or so (low levels), so the 25-hydroxyvitamin D peak is probably all of February.
The best innate and adaptive immune responses, and the lowest risk of dysregulated hyper-inflammatory responses, are likely to occur over February. The first two directly reduce disease severity, and so total viruses shed per infected person - and so transmission. This strongly affects the total number of newly infected people.
New infections take a week or so to be diagnosed and reported. With widely available home tests, PCR tests and official reports will increasingly under-estimate the real infection numbers, since many people would be reluctant to report their infected status to the government . . . . unless they want to get their infected status officially recognised, in order to (in potential future arrangements) to avoid the need for vaccination and/or to avoid restrictions placed on the unvaccinated and those who are deemed not to have been infected yet.
Those (most of whom have inadequate 25-hydroxyvitamin D and no access to early treatment) who develop serious symptoms typically need hospitalisation 2 to 4 weeks after the initial infection. Deaths probably occur another few weeks, to two months, later.
The race/ethnicity of COVID-19 hospitalised patients in Australia is rarely discussed in public. It is well known that the NSW Delta outbreak started primarily in the western and south western suburbs of Sydney with the highest proportion of people whose first language was not English (ABC): (Fairfield, Liverpool, Canterbury-Bankstown, Cumberland, Parramatta, Blacktown, Georges River and Campbelltown). I can’t find the link now, but the most common non-English language spoken in these local government areas is Arabic.
Police and military personnel patrolled the streets of these areas to enforce lockdowns, the new home of many people who came to Australia to flee oppressive military governments in the countries in which they were born. For instance, in NSW in September 2021, police dispersed, arrested and fined Muslim mourners who attempted to watch a funeral while remaining in their cars.
Sydney and Melbourne are Australia’s two most populous cities, and have the greatest numbers of recent immigrants, many of whom have somewhat darker skin than Australians of European descent, with those from Ethiopia and Somalia having very dark skin. This melanin (and I recall some other compound not so visible, which is also found more in darker skin) reduces the ability of ~295nm UV-B light to penetrate far enough into the skin to the cells in which 7-dehydrocholesterol is converted to vitamin D3 cholecalciferol.
So these recent immigrants AND many Indigenous Australians (who have also suffered high rates of COVID-19 transmission and severity in some towns and rural settlements) are at a great disadvantage regarding 25-hydroxyvitamin D levels, unless they supplement D3 properly, due to requiring a greater amount of sun exposure for their skin to produce the D3 they need.
For Muslims, most of whom have immigrated in the last decade or so, an additional problem, at least for many of the women, is the cultural practice of all-covering clothing at all times, and so allowing very little skin exposure to the sun. The year-round average 25-hydroxyvitamin D levels of Arab (primarily Muslim) women in sunny Israel is disastrously low, with some of them falling below the 4ng/ml detection limit. This shows in the lowest bar being higher than the trend line.

The link between vitamin D deficiency and Covid-19 in a large population Ariel Israel et al. 2020-09-07 medRxiv preprint.
It is reasonable to expect similarly low levels for Muslims in Sydney NSW (New South Wales - a daft name for an Australian state) which is at 33° south, while Jerusalem is at 31° north. In Melbourne, Victoria (37° south), we might expect similarly low levels most of the year, and significantly lower levels than in the above graph in winter and spring.
For those who understand the importance of 25-hydroxyvitamin D, it will come as no surprise that (ABC 2021-10-10) that most of the COVID-19 hospitalised patients were from “Culturally and Linguistically Diverse” (CALD) backgrounds. The hospitalised numbers are not disclosed, but Doctor Mark Putland said:
. . . the majority of the Royal Melbourne Hospital's last 350 COVID-19 patients in the emergency room were from a CALD background.
Low 25-hydroxyvitamin D levels are not the only cause of this illness, suffering and death. These recent arrivals often have large family groups living in dense, lower-cost, housing. Furthermore, their fear of governments, and some Victorian government actions involving police and stark, emergency COVID-19 treatment centres set up in warehouse-like buildings, has made many people reluctant to seek medical care. Dr Mark Putland again:
CALD patients are also presenting to hospital late.
"What we hate to see is an avoidable tragedy … when we have someone turn up to a hospital gasping their last breath with a disease that we could have treated," he says.
"Tragically, we have had cases that were kind of just a moment too late."
Dr Putland says CALD patients may understandably be frightened of encountering the health system.
"It doesn't matter if you're rich or poor, if you've got a visa or or passport or, or you're an Australian citizen …. All we want to do is take care of people."
This article features several people from African (Somalian) and Arabic backgrounds.
There is a bigger avoidable tragedy here which Dr Putland is unaware of. It has long been obvious to vitamin-D aware people that these darker skinned and/or sun-avoidant people would benefit enormously from proper vitamin D supplementation - along with the elderly, and those suffering from obesity.
No less of an authority than the Head of the Department of Medicine, at Monash University, long-time vitamin D researcher Professor Peter Ebeling, stated this, in an ABC News interview in August 2020.
As far as I know, nothing like this has been done. Any such preventive action would undermine the legitimacy of the official program of vaccines to the exclusion of all other approaches, until hypoxia sets in and hospital treatment is required. (The sole exception to this is expensive, invasive, medically administered monoclonal antibody treatment, particularly in the USA.)
I emailed vitamin D information, links to my sites and to other sites, etc. to both Dr Putland and the imam of a Melbourne mosque who was featured in this article. As usual, I received no reply.
This is a long way of supporting my suggestion that the hospitalised people in Victoria during December 2021 are still probably disproportionally drawn from the subset of the population who have the lowest 25-hydroxyvitamin D levels.
This is so easy to fix! Part of the trouble is that D3 capsules in Australian stores are 1000IU, which sounds like a lot. Five of these are day are needed for 70kg bodyweight, and probably ten of 15 for adults suffering from obesity: vitamindstopscovid.info/01-supp/ . This is distasteful, awkward and involves excessive amounts of vegetable oil (we already have too much omega 6 fatty acids in our diet).
Other than getting 50,000IU dry capsules from the USA, including via Australian eBay sellers, it is possible to get a good deal on 10,000IU oil-filled capsules, or tablets, if you know where to look. For instance, Australian seller wavetunes can provide a bottle of 360 10,000IU Bronson tablets for AUD$35 (~USD$25) including shipping: https://www.ebay.com.au/itm/174976826522. At one every two days, this is enough for two adults for a year.
Most people look at the terrible toll of suffering, harm and death from COVID-19 as being tragically inevitable. Vitamin-D aware people view this as an egregious failing of public health, since almost all of these people would not get very sick if they spend something like AUD$18 a year on D3 supplements.
In the USA, the same product, direct from the bronsonvitamins eBay store (99.8% positive feedback), costs USD$15 with shipping.
~ ~ ~ ~ ~
There are new developments regarding harm from the current mRNA and adenovirus vector COVID-19 vaccines but I don’t have to do more than link to them:
Myocarditis after vaccination, by type and timing, in Ontario www.medrxiv.org/content/10.1101/2021.12.02.21267156v1. Dr Vinay Prassad regards these levels as alarming.
Time to punish the UK 5 million COVID-19 vaccine refusniks.
The best analysis I have seen of the rise in sports players and athletes collapsing and/or suffering heart attacks: goodsciencing.com/covid/71-athletes-suffer-cardiac-arrest-26-die-after-covid-shot/ .
Search for "vaccine injured" on Google, Duck Duck Go and Russian Yandex - which seems to have the most alarming links. To what extent each such item is valid I can’t say without a great deal of work. According to University of Zurich research Google presents the least conspiracy theories (their test terms look like BS to me) and Yandex the most. So Yandex might be good way of finding material which makes the currently dominant people in the West most uncomfortable, while recogising that quite a lot of the links might be to sites containing utter crap.
“vaccine dead” Google. "vaccine dead" protests images at Yandex.
A Nutrition Matters reader kindly supplied a photo he took in London on 2021-12-08, of a protest outside a pub on Westminster Bridge Road, opposite the Houses of Parliament, depicting people who had apparently been killed by COVID-19 vaccines:
~ ~ ~ ~ ~
There are new developments regarding harm from the current mRNA and adenovirus vector COVID-19 vaccines but I don’t have to do more than link to them:
Myocarditis after vaccination, by type and timing, in Ontario www.medrxiv.org/content/10.1101/2021.12.02.21267156v1. Dr Vinay Prassad regards these levels as alarming.
Time to punish the UK 5 million COVID-19 vaccine refusniks.
The best analysis I have seen of the rise in sports players and athletes collapsing and/or suffering heart attacks: goodsciencing.com/covid/71-athletes-suffer-cardiac-arrest-26-die-after-covid-shot/ .
Search for "vaccine injured" on Google , Duck Duck Go and Russian Yandex - which seems to have the most alarming links. To what extent each such item is valid I can’t say without a great deal of work. According to University of Zurich research Google presents the least conspiracy theories (their test terms look like BS to me) and Yandex the most. So Yandex might be good way of finding material which makes the currently dominant people in the West most unconfortable, while recogising that quite a lot of the links might be to sites containing utter crap.
”vaccine dead” Google. "vaccine dead" protests images at Yandex.
A Nutrition Matters reader kindly supplied a photo he took in London on 2021-12-08, of a protest outside a pub on Westminster Bridge Road, opposite the Houses of Parliament, depicting people who had apparently been killed by COVID-19 vaccines:

@WrightWayUK appears to be an Instagram hashtag related to Dr Stephen Wright, a 32 year old child psychologist and father, who died after receiving the AstraZeneca vaccine: The Independent and a video by his sister-in-law.
Deaths caused by the Astrazeneca adenovirus vector vaccines are well known and recognised. Baker et al. 2021-12-01 www.science.org/doi/10.1126/sciadv.abl8213 suggest the problem may be related to the chimpanzee-derived adenovirus, rather than the COVID-19 specific instructions it carries into cells to make them produce the spike protein. Perhaps this would happen less if vaccinators aspirated the needle to reduce the chance that the vaccine goes into the bloodstream. See my comments on this Vinay Prassad article.
U06 2021-12-16 Omicron: Tentative evidence of lower severity from University of Hong Kong in-vitro experiments
12 days has passed since my original article, and we do not yet see clear signs of hospitalisations due to Omicron being in the same proportion to the very rapid rise in Omicron cases in comparison to Delta. However, there has hardly been time for this in countries 30° or more north of the equator - so I think there is not yet any epidemiological support for Omicron causing generally less severe disease in these generally vitamin D deficient and early treatment deprived populations.
The first tentative mechanistic evidence for Omicron’s virulence being less than that of Delta arrived on 2021-12-15 from the University of Hong Kong:
www.med.hku.hk/en/news/press/20211215-omicron-sars-cov-2-infection
The researchers found that over a single day in cell cultures, Omicron grows 70 times more than Delta in bronchial tissue - the two pipes which carry air to and from the lungs. This is the difference in height, in these log vertical scale graphs, between the leftmost Delta bar and the leftmost Omicron bar.

However, looking at 48 hour growth bars in their graphs, I estimate that in two days:
Omicron grew 1.8 times as much as Delta in bronchial tissue.
Omicron grew 0.53 times as much as Delta in lung tissue.
There are numerous other factors which affect how infection progresses in each person, including especially the actions of the immune system, which played no role in these experiments.
To the extent that real-life infection follows these patterns we might expect:
Greater transmissibility due to more viruses being available in the bronchi to be swept up in the outgoing high-velocity air as we exhale.
Lower severity due to less growth in the alveolar (tiny air sacs) tissue where the infection itself and the resulting (potentially dysregulated, hyper-inflammatory) immune responses cause the worst trouble which leads to severe COVID-19: destruction of the endothelial cells in the capillaries (the cells which line the smallest blood vessels) where oxygen and carbon dioxide exchange occurs, leading to hyper-coagulative blood and so to still further disruption, fluid discharge, hypoxia (low blood oxygen level) and damage to all organs due to microembolisms and larger clots.
~ ~ ~ ~ ~
We have enough trouble in northern European countries (here counting the UK as “European”) with deaths due to Delta rising as vitamin D levels fall towards their ~ January and February winter nadir: ourworldindata.org:

See my article on seasonality and vitamin D.
Assuming Omicron displaces Delta, if it is more transmissible and (in all the terrible circumstances) equally harmful, then we are in bigger trouble than last year.
Omicron is much more transmissible - doubling every 3 days or so. So the number of infections will rise probably higher than in the past (though these PCR tested case numbers do not show all infections) and Omicron would need to be a lot less likely to cause serious disease, if the outcome is going to be no worse than in the past.
Numerous factors are at work. The most vulnerable have died or acquired good immunity, which Omicron will be able to escape to some degree in terms of infections, and hopefully will be less likely to escape in terms of severe symptoms.
So the age-distribution of those most likely to be infected this northern winter is likely to be younger than last winter, which should, with luck, reduce the incidence of harm and death - while making all such harm and death more of a burden due the greater number of life years lost or curtailed.
U07 2021-12-17 South African video bulletin
I have not had time to listen to the whole presentation earlier today www.youtube.com/watch?v=rBi503tCZis, but here are two images of interest:

(37:00) In Western Cape province, a lower ratio of hospital admissions to PCR detected cases than in the Delta wave, attributed to increased infection-acquired and vaccine-induced immunity.
In an unvaccinated person with no previous infection, no evidence to date that Omicron is less severe than previous variants.
We are still seeing some very sick patients.
So Omicron only escapes immunity from vaccines and Delta (and other prior variants) to some degree.
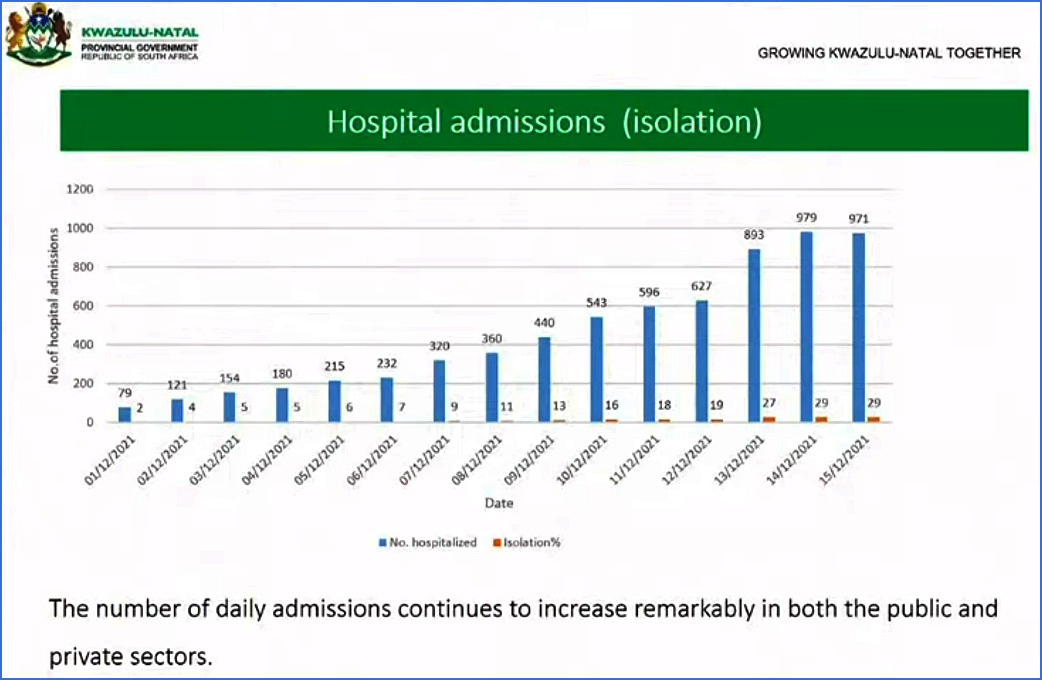
(47:00) In Kwazulu-Natal province, hospitalisation admissions have risen from 79 to 979 in two weeks.
U07 2021-12-20 Deaths in the UK and 2 day doubling times; Ivermectin widely used in South Africa
From 16th December data in the UK, Reuters reports 7 deaths due to Omicron and cases jumping from 10,000 to 25,000 in 24 hours.
The numbers of new Omicron cases per day in Gauteng province, South Africa, are no longer growing but they are in other South African provinces: Gauteng has not reported hospitalisation data since 4th December: gpcoronavirus.co.za/#cases/province.GP/Hospitalisation.
Here in Victoria, Australia, cases and hospitalisations are rising - and this is mainly Delta, as vitamin D levels rise towards their (as best I know) February peak. There is is some Omicron here and it is surely growing, but I don’t think it has yet strongly influenced case numbers and hospitalisation: www.abc.net.au/news/2021-12-20/victoria-covid-cases-and-deaths-melbourne-testing-site-wait/100713112.
16th December Washington Post: Omicron cases doubling every 2 days.
In the sunny, and largly COVID-19 un-infected, Australian state of Queensland, Omicron cases have a 2 day doubling time.
San Diego wastewater surveillance shows 3M RNA detections per litre, which is 3 times the level at the peak of the Delta wave: youtube.com/watch?v=RuCEYez1Klg and rising much faster than Delta. “You poop it out before you get symptoms.”.
A South African writes to Steve Kirsch: “Ivermectin, zinc and aspirin saw us through the first infections. To be honest, most of us have the sheep dip version available freely at the farmers cooperative!” and “Most people can’t afford the tests and they can’t afford to lose their incomes from taking time off work. Middle class suburban moms might still be testing but the rest of us are done playing silly games.”
U09 2021-12-23 Nothing conclusive regarding virulence
I see nothing conclusive yet about the severity of Omicron vs. Delta in populations with low vitamin D and no access to early treatments. There are some indications of it being milder, but it is too early to tell, and there can be no precise experiment since the natural and vaccine-acquired immunity status of populations has changed since the start of the Delta wave, as well as their 25-hydroxyvitamin D levels.
The maniacal focus on vaccination is abundantly clear in President Biden's 2021-12-21 speech:
In the first 13 minutes he used the words vaccinat(e/ed/ion), boost(er/ed) or, separately, shots, 76 times - about once every 10 seconds. There was no mention of:
* Infection acquired immunity.
* Dangers of vaccination.
* Early treatments, all of which except monoclonal antibodies and new expensive concoctions of multinational pharmaceutical companies are disparaged or banned.
* Nutrition.
* Action to reduce or at least recognise co-morbidities.
* Why anyone who has already been infected should subsequently be vaccinated.
At the end, when taking questions, he became angry about parents being required to pay exorbitant prices, such as USD$500 a month, for insulin on which their child’s life depends. Yet there was was no mention - even in the questions from the press - of the US government, via its FDA, NIH and CDC agencies, preventing people from using ivermectin in early or hospital treatment for COVID-19.
The Guardian reports WHO Director General Tedros Adhanom Ghebreyesus PhD argued against booster doses to combat the Omicron wave - because he wants the limited number of vaccine doses to be used in countries other than the developed ones where many people have already had their initial (usually two) doses. Yet everywhere else people are being exhorted to get vaccinated, and if vaccinated, to get a booster injection.
WHO epidemiologist Maria Van Kerkhove [WP] cautioned against reports of Omicron being less virulent, saying there was still insufficient data to make a judgment. “We have not seen this variant circulate for long enough in populations around the world, certainly in vulnerable populations.”.
COVID-19 vaccines are only a year old, yet Israel has long been offering (and requiring?) a booster (3rd injection) in addition to the initial two Pfizer injections which made the person, for a while, that much desired fully vaccinated. Now, Israeli authorities are offering a second booster, the 4th injection, to those who are over 60, have compromised immune systems or are healthcare workers, four months after their booster injection. Reuters 2021-12-23. The minimum time between the second dose and the third (the first booster) was reduced from 5 to 4 months.
A UK report indicates that Omicron leads to fewer hospitalisations than Delta: www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-50-severity-omicron/. I have not had time to read the report. My guess is that this is a substantial indication that Omicron is less virulent than Delta in the UK population, most of whom are highly vulnerable due to very low 25-hydroxyvitamin D levels and no access to early treatment, but many of whom have infection acquired immunity or some degree of immunity from vaccines.
With such low 25-hydroxyvitamin D levels and no early treatment, many people who do not recognise these problems and do not know that they can and should be fixed, think that vaccines are a great wonder because they provide significant protection against severe disease, and moderate but rapidly declining protection against infection in an environment in which so many people are being harmed and killed.
Barda et al. 2020, an Israeli survey of myocarditis rates resulting from the Pfizer COVID-19 vaccine and from COVID-19 infection, published on 2021-09-16 was updated with data stratified by sex and age being below or above 40 years: www.nejm.org/doi/full/10.1056/NEJMc2115045 . Briefly: vaccination causes myocarditis mainly in younger males, with ~8.62 events per 100,000 males aged 16 and 39. Infection increased risks for both sexes in all ages, with ~11.54 events per 100,000 males and females aged 16 to 39. The researchers caution that the confidence intervals are wide, meaning that the results are not necessarily an accurate representation of what actually occurs.
The table covers multiple other adverse outcomes such as shingles and heart attack. Even with this 888,828 person dataset the data is quite thin and would require more expertise and patience than I have to properly interpret. A statistician would be able to estimate significance for the various results.
My impression is that Israel keeps better medical records than most countries. Assuming, tentatively, that the Israeli observations of adverse events from the Pfizer COVID-19 vaccine were broadly representative of those in other countries where Moderna (like Pfizer but ~3 times stronger, I recall reading), AstraZeneca and J&J vaccines are also used, the challenge is to reconcile these observations with the reports, analysis, beliefs and statements of those who believe that the harm caused by vaccines is very much higher than officially recognised.This would be a huge task. I am trying to show some of the reasons why many people are alarmed about these vaccines, and at least some of what may be substantial evidence or arguments to the contrary.
I have enough concerns about these mRNA and adenovirus vector vaccines causing cells - potentially anywhere in the body, to sprout spike proteins and so be attacked and destroyed by the immune system, with potentially unknown complex immune system consequences.
We could place more trust in observations and analysis such as in this Israeli article if the COVID-19 vaccination program in Western countries was responsible, and properly situated as a subset of a larger program which focused on nutrition and early treatment. But in fact, the program is utterly reckless and at odds with those superior approaches. I plan an article devoted to how reckless the program really is, to follow an article on research which shows, beyond a shadow of doubt, that influenza vaccines have no impact on hospitalisation or deaths for UK people in their 60s.
Steve Kirsch is one of the best known proponents of concerns about COVID-19 vaccine safety. If you subscribe to his Substack, you won’t miss much in this regard.Do the graphs shown in this article nakedemperor.substack.com/p/correlation-between-increased-mortality show increased rates of death not for unvaccinated people in older age groups in the UK, not within 21 days of the first vaccination, not after the second injection, but between 21 days after the first injection and the second? It looks like it - but it would take me a day or so to research the matter properly.
A peer reviewed article on three cases of thyroiditis caused by mRNA COVID-19 vaccination.
Canadian authorities recommend 2021-12-03 (page 7) that 18 to 29 year olds get the Pfizer vaccine and not the Moderna one due to the higher incidence of myocarditis with Moderna. The two are apparently very similar, with the Moderna containing about three times as much material.
Steve Kirsch provides a list of 291 sports people who have collapsed, with each items supported by a link to a news or other site. This was apparently generated by someone (ex-CIA we are told) who was asked to research reports of a rise in athletes’s collapses, heart attacks and deaths.
This, with its rise in July to November, seems to support the analysis mentioned above: goodsciencing.com/covid/71-athletes-suffer-cardiac-arrest-26-die-after-covid-shot/. I don’t have time to investigate. Others are on the case. How to check the validity and significance of any such apparent increases?
Here is another article raising such concerns. This article claims that Wikipedia stopped listing the soccer players who died during play.
This Associated Press [WP] article which argues that some of the videos of sports people collapsing were taken before COVID-19 vaccines were available, or were of people who had not been vaccinated. Such a critique can’t necessarily show that a larger body of such claims do not represent a genuine trend, but it shows that we should not accept claims about such trends without careful research. But who has the time for this?
An argument for the validity of these claims is that the pro-vaccine authorities have ignored them - and we already know the impetus behind the vaccines is reckless and ill-informed as to the dangers and to the better alternative of early treatment, even if these people have never heard of vitamin D.
So as Christmas approaches we find a video showing people collapsing on the sports ground, in the classroom, at work and at home . . . people twitching on the ground as others rush to palpitate their hearts . . . all to a skillfully sing jolly rendition of a Christmas song which tells us that the government wants to kill us: It’s Beginning to Look a Lot Like . . . . Genocide: www.bitchute.com/video/sqTd8LtViqI0/ . Not all the commenters agree that this is a valid assessment of vaccine adverse events, but there are 916 thumbs up and 32 down.
The polemics of BitChute are hell-and-gone from careful, well-referenced, research and discussion, but when I see how maniacal the push for vaccines is, and how strongly anything to the contrary is suppressed in conventional channels of communication, I wouldn’t rule out the possibility that we might find some elements of an ugly, tragic, truth in less censored places, where passions, ignorance and stupidity flow freely. Some of these passions are well based in frustration, fear and horror of this man-made disaster which has been forced on everyone as if it is the best possible response to the pandemic.
U10 2021-12-24 Encouraging statistics from London hospitals that Omicron is less virulent than Delta
This article is worth reading in full:
dailysceptic.org/2021/12/23/a-doctor-writes-an-omicron-tsunami-is-coming-isnt-it/
A doctor in London presents graphs depicting statistics to 21st December from London hospitals - and London is the epicentre of the Omicron wave in the UK. Although prior infection rates may be higher in London than in other parts of the country, and while most of the country is still further north, and so lower in vitamin D in general,

(Sutherland et al. 2020: sci-hub.se/10.1016/j.clnu.2020.11.019.)
it is a large, dense, city in winter where many people have extremely low vitamin D levels, and no access to early treatment.
Hospital admissions for COVID-19 are rising, but ICU numbers are falling.
The proportion of people who are in hospital and COVID-19 positive (presumably mainly with Omicron) but who were admitted for another reason is rising faster than the number of people were were admitted because their COVID-19 symptoms are serious enough.
It is early days, but by mid-January the observations in London will probably give us a realistic estimate of Omicron’s virulence in the vulnerable populations of most northern hemisphere countries more than 30° from the equator this winter.
Ideally, a variant would arise which is highly infectious, confers lasting immunity for all likely future variants, and causes no harm and only minor symptoms. This might be true of Omicron when people have 50ng/ml 25-hydroxyvitamin D and access to several good early treatments - except that its transmission might then be greatly reduced with R0 below 1.0 except within homes and other very physically closely integrated sub-populations, such as those in hospital, aged care homes and prisons.
That would be a good outcome: low levels of transmission, little serious disease, no overload of hospitals, everyone getting early treatment followed by the excellent treatment in hospital, hopefully requiring little in the way of corticosteroids (such as prednisolone and dexamethasone to suppress excessive inflammation) and little or no use of ventilators.
Vaccinations would generally be worth their inherent risks only for those with significant co-morbidities. If Novavax becomes available - it has just been approved to some degree in Europe - this surely has fewer risks than the current vaccines, so it wold make sense to use it more widely.
Hands up those who recognised the handsome doctor whose colour portrait heads the DailySceptic article! This is Dr Beaker, of Supercar [WP], the early 1960s Gerry Anderson series. I watched this 60 years ago just after my family arrived from England in our new home, Australia. New revelations about the origins of Doctor Horatio Beaker are at: www.gerryanderson.com/fab-facts-supercars-dr-beaker-was-created-for-a-different-tv-show/ .
I look forward to a future in which nutrition for all humans - and our companion animals, horses and agricultural animals - is, as Dr Beaker would say, Most Satisfactory - as he does at the end of this video.
U11 5th January 2022 - Omicron seems to be less virulent
A great deal has happened in the last two weeks. As is now well known, Omicron is very transmissible and is ramping up case numbers in many countries, including here in Australia, but also the USA and the UK.
With one exception, all indications seem to be that Omicron causes significantly less hospitalisation than Delta - such as 50% - in broadly similar populations far north of the equator this northern winter.
The exception is that children are being hospitalised with COVID-19 at much higher rates than in the past: www.khou.com/article/news/health/coronavirus/texas-childrens-covid-cases-double-babies-icu/285-8f06a236-cc0f-40a4-aaab-4bb5b535f6f9 This is a report on the rising number of children being admited to the Texas Children’s Hospital with COVID-19. I wrote to Dr. Jim Versalovic about vitamin D. No reply yet . . .
The Omicron wave is subsiding in South Africa - so the actual number of cases is surely many more than those counted in official PCR tests. This variant quickly infected so many people who were vulnerable to it that the number of such people remaining, uninfected, declined within weeks to the point where such growth rates were impossible.
It seems that in Australia many people who want a PCR test can’t get one, so the actual case numbers very much exceed the official count, which itself is skyrocketing far beyond the previous relatively small waves. From www.abc.net.au/news/2022-01-05/victoria-new-covid-cases-deaths-hospitalisations-ambulance/100738680 2022-01-05, here in Victoria, Australia:

NSW (pop. 8.2M) has much higher official new case rates - 35,054 a day, with only a subset of people wanting to be tested actually being tested, and with multiple day delays in results commonplace. The authorities are now discouraging people from getting a PCR test, such as by stating that if they test positive with a home-based rapid antigen test, that they should not get a PCR test. This means the government is not trying to find out who is infected. They should, since they should not expect any person with infection acquired immunity to participate in their vaccination drives (which are ramped up to fever pitch regarding boosters at present) or be excluded from travel, hairdressers, concerts, cafes etc. when not recently vaccinated.
One hypothesis is that Omicron is better adapted to replicating in the airways and less in the lungs relative to prior variants, which makes it more transmissible and less likely to cause severe COVID-19. To the extent that this is true - and I think we can assume this to be generally the case - then Omicron is arguably a blessing, since it out-competes other variants which generally cause more serious disease in the generally vitamin D deficient populations who have no access to early treatments.
~ ~ ~ ~ ~
So what happens when 50%, 70% or 90% of the population, children included, have been infected by March or so?
Why would they want to keep getting COVID-19 vaccines or boosters? There is no reason for them to do so. The vaccination program should stop, except for a handful of people who, even with good vitamin D and early treatment, are at such risk of serious COVID-19 with Omicron that the risks of the vaccines are worth it for the protection they provide.
How much protection does a early-2020 model spike protein mRNA or adenovirus vector “vaccine” provide against serious outcomes from Omicron? Any protection is welcome, provided the person themselves decides that the risks of “vaccination” are worthwhile in all the circumstances.
~ ~ ~ ~ ~
Be sure to read the U12 section below on arguments concerning the hypothesis that deaths and disability in working age people in the USA rose, especially in the 3rd quarter of 2021, due to the ill-effects of COVID-19 vaccines.
There is a new angle on the COVID-19 “vaccine” injury and death debate. It first surfaced as an article, which cited no sources, about the CEO of an Indiana-based insurance company stating that in the 3rd quarter of 2021 (and continuing into the 4th) that deaths among 18 to 64 year olds were 40% above pre-pandemic levels, and that this was very much more than would be expected from official COVID-19 deaths in this age group. The article is: www.thecentersquare.com/indiana/indiana-life-insurance-ceo-says-deaths-are-up-40-among-people-ages-18-64/article_71473b12-6b1e-11ec-8641-5b2c06725e2c.html
The CEO is J. Scott Davison: www.oneamerica.com/newsroom/leadership/scott-davison .
Several people wrote this up, most prominently Steve Kirsch: stevekirsch.substack.com/p/unprecedented-deaths-in-indiana-for
Mathew Crawford wrote about it to some degree on 2022-01-03 roundingtheearth.substack.com/p/why-are-non-covid-deaths-at-historic and linked to the page with the video: fox59.com/news/coronavirus/indiana-chamber-of-commerce-and-indiana-hospital-association-to-hold-news-conference-on-covid-19-situations/
Next, in an article published in two locations: rescue.substack.com/p/chilling-pandemic-data-from-the-insurance and trialsitenews.com/chilling-pandemic-data-from-the-insurance-industry/ (this lacks the diagram, which is in the rescue.substack.com article). This article is at the site of Michael Capuzzo who wrote so beautifully about ivermectin in May 2021. The article is by another celebrated author, Mary Beth Pfeiffer (Google).
She approached OneAmerica about what their CEO Scott Davison said in the video, and received a statement with a graph. The numbers in the statement - at least as she reported them - do not not look right in one important respect. I am inclined to think that the fears of very high deaths in the 3rd quarter of 2021 among US 18 to 64 year old working people are well based. To what extent they reflect the ill effects of COVID-19 vaccines is not so clear. However, this line of enquiry strikes me - and many others - as worthy of further attention. Here is what I wrote in comments to this article, in both its locations.
The video is at fox59.com/news/coronavirus/indiana-chamber-of-commerce-and-indiana-hospital-association-to-hold-news-conference-on-covid-19-situations/
Here is my transcription of what Scott Davison said in the two segments (of four) in which he spoke about these death rates:
(23:10)
One of our business is we offer group life and disability insurance to employers. We are seeing, right now, the highest death rates we have ever seen in the history of this business. Not just at OneAmerica - the data is consistent across every player in that business.
This is primarily working age people, 18 to 64, that are in employers like those employers on the screen here.
What we saw just in 3rd quarter - and we saw it continue into 4th quarter - is that death rates are up 40% over what they were pre-pandemic.
Just to give you an idea of how bad that is, a 3 sigma [3 standard deviations] or a 1 in 200 year would be a 10% increase over pre-pandemic. So 40% is just unheard of.
So what the data is showing us is that the deaths which are being reported as COVID deaths greatly understate the actual death losses among working age people from the pandemic. It may not all be COVID on their death certificate, but deaths are up just huge, huge, numbers.
We are also seeing an uptick in disability claims. At first it was short-term disability claims and now we are seeing long-term disability, whether it is long-COVID, whether people haven't been able to get the healthcare they need because the hospitals were overrun.
For OneAmercia, we expect the costs of this will be well over 100 million dollars - and this is our smallest business. So it is having a huge impact on that.
Those costs will trickle towards other employers, because premiums are starting to go up - so it will cost more for employers. Most of us in the industry are starting to target and add premium loads on employers who are based in counties which have low vaccination rates. Its typically what we would in underwriting when we have a risk factor like that.
There is also going to be higher costs on employers due to greater absences, particularly at a time when there is low unemployment and workers are hard to come by. But they will be out because they are sick, because they have long-term disability or sadly they have passed.
(34:40)
I am not suggesting that the COVID deaths are under-counted - but the pandemic related deaths indicate much larger death rates among working age people than simply COVID on the death certificate would imply.
So what we are seeing is that people get COVID, they kinda recover, and then they die from some sort of disease mechanism that was impacted by the fact that they got COVID in the first place.
So we are seeing this massive number of deaths - and it's across the industry, its not just OneAmerica numbers, this is consistent across every carrier in every state that does business in this industry.
So we would say that the pandemic-related deaths are much larger than what you are seeing in the news as the official, specific COVID deaths, where COVID was the proximate cause of death on the death certificate.
So it's a much, much larger number than that.
We've got 40 to 46% up just in the 3rd quarter alone from the Delta wave.
Here is the graph from Mary Beth Pfeiffer’s article for easy reference:

The following assumes that you have read the article. I am referring to the final paragraph of the article, which is apparently the final paragraph of the statement from OneAmerica:
Additional detail regarding the 40 percent increase in death rates
The graph, which represents publicly reported death rates from the CDC for 18-64 age groups from 2019-21, demonstrates trends and the significant impacts of COVID-19. Based on the U.S. population, there are an estimated 200 million people between the ages of 18 and 64. CDC statistics (in green) show the baseline pre-pandemic death rates in the center of the graph, listed at 100%. The blue line, representing 2020 trends, begins to show COVID impact in Q2 of 2020. The black line represents 2021 deaths in this age group and peaks in Q3 (with the most recently available data through the end of Q3). Using actual CDC reported death totals, 2019 (pre-pandemic) recorded 172,000 deaths during that three-month period. CDC data from Q3 2021 shows 250,000 actual deaths (or a 45% increase over the baseline expectation) for this age group, typically the working age population. Of that total, 50,600 were attributed by the CDC to COVID.
Does 50,600 sound like the correct number of COVID deaths in the USA in the 18 to 64 age group for Q3? No:
US cumulative COVID-19 deaths at: ourworldindata.org/coronavirus/country/united-states shows 2021-06-01 594,357 and 2021-09-01 642,908 = 51,449 for all ages, Q3.
So this 50,600 figure does not even resemble the Q3 deaths for 18 to 64 year olds. I don't have a quick way of determining this, but the figure of 25% of deaths being in this age group sounds reasonable. Guesstimating 12,750 deaths in that age group, than the figures quoted in the above statement look more alarming than the statement indicates, and are compatible with what Scott Davison said in the video. (BTW, he gave me the impression that he knows what he is talking about.)
(In the top graph at: www.usmortality.com, turn off Smooth and turn on Maximize.

Using the cursor on the graph, the excess deaths per week peak at 19,419 on week 35 at the end of August to start of September.)
In the figures apparently supplied by OneAmerica, 250,000 18-64 deaths in Q3 exceeds the 2019 figure of 172,000 by 78,000, which is 45.3% higher. So far, this accords with Scott Davison's statements.
My guesstimate of 12,750 COVID-19 deaths is just 16.3% of this 78,000. That accords with what he said too - that the official COVID-19 deaths are a small fraction of the supposed 78,000 excess deaths in this quarter in this age range.
Some of the remaining ~~83% of these 78,000 deaths are surely due to longer-term effects of COVID-19, but it would be surprising if this was more than a small fraction of the ~~12,750 deaths. This leaves a large unexplained gap. Scott Davison was not thinking at all that these might be caused by vaccination. He seems to assume that they are mainly a result of severe COVID-19 - and severe symptoms without death scales in rough proportion to deaths in any population. He and his underwriting colleagues assume, not unreasonably, that deaths and so severity and later deaths are in inverse proportion to vaccination rates. (In the criminally egregious absence of proper 50 ng/mL 25-hydroxyvitamin D levels and banning of early treatments, vaccination does very significantly reduce severity and deaths.)
What we really need is age-stratified death information, ideally with individual vaccination and prior COVID-19 illness data. That may not be available, so we might be able to get monthly excess deaths, in some band of ages, and then subtract official COVID-19 deaths, to leave the unexplained deaths we suspect were caused in large part by vaccination. Then we need to get that data, by month, ideally state-by-state, and see how it correlates with 1st, 2nd and subsequent COVID-19 vaccine injections.
Please remember that these so-called vaccines, even if they worked as well and were as safe as claimed, would still be a distant third best way to tackle the COVID-19 pandemic, after population wide vitamin D supplementation to attain at least the 50 ng/ml 25-hydroxyvitamin D level the immune system needs to function (most people have 1/2 to 1/10th of this) and, in second place, multiple early treatments.
I have written above of some of the material I have seen regarding reports of injuries and deaths which are ostensibly caused by the mRNA an adenovirus vector COVID-19 “vaccines”. I do not have the time to research this in great detail. However, I find quite a lot of this worrying - and it seems to tie in with MSM (mainstream media) reports late in 2021 being unaccountably full of people with heart and breathing difficulties - which were not associated with COVID-19.
I can’t give anyone solid guidance on this. It would not surprise me if there are a great deal more injuries and deaths from these treatments than are currently officially recognised. We live in a time of mass hysteria with most people fervently believing that vaccines are the only way of saving themselves and society - so the believe it is justifiable and necessary to encourage (to the point of forcing) everyone to get vaccinated. A major part of this is that they dispute the veracity of any alternative to vaccines, believing that any beliefs along these lines will reduce the number of people who are vaccinated.
I believe that a major reason why vitamin D, other nutrients and early treatments have been maligned and/or outright banned by most governments and the majority of the population is that most people have been whipped along in their fears and herded by most governments, the mainstream media and multinational pharmaceutical companies.
In solving the problem of the suppression of nutrition and early treatments, we have to face the enemy - which is primarily an irrational and highly manipulated excessive faith in, and feeling of dependences upon, vaccines in general and especially these mRNA and adenovirus vector COVID-19 so-called vaccines. Part of this story is the fervent rejection of these “vaccines” by a minority of the population including some health professionals.
A major new development in this debate is the 3 hour interview of Dr Robert Malone, MD, by Joe Rogan:
Dr Malone developed the crucial principles which mRNA “vaccines” are based on. I have not listened to this yet, but from all accounts, it is essential listening for anyone concerned with the disastrous response to the pandemic, and so the COVID-19 Vaccine Civil Wars which currently split many families and former friendship groups.
This war spans classes, cultures, countries and continents (no alliteration intended!). The eventual losers are digging in hard: www.zerohedge.com/political/french-president-views-unvaxxed-non-citizens-vows-piss-them President Macron is quoted as saying, in English translation:
“I am not about pissing off the French people,” Macron told the readers of Le Parisien on Tuesday.
“But as for the non-vaccinated, I really want to piss them off. And we will continue to do this, to the end. This is the strategy.”
He declared that “worst enemies” of “democracy” are “lies and stupidity,” then declared that his government is “putting pressure on the unvaccinated by limiting, as much as possible, their access to activities in social life.”
Macron’s government claims that 90% of its citizens are vaccinated. He promised to “reduce” this minority with further restrictions.
The current disastrous situation defies easy description. The apparently generally lower virulence of Omicron is a stroke of luck. Despite popular opinion to the contrary there is no reason why a more transmissible virus generally would be less virulent.
Omicron is sweeping through many countries - and will hopefully create lasting immune responses which will suppress the transmission (ideally) and severity (we fervently hope) of future SARS-CoV-2 variants.
This is going to be a wild ride, in many aspects of disease, politics, public policy and recriminations against those who pushed vaccines to the exclusion of all else.
How are the majority of the medical profession going to be respected after all this settles down? The vaccines will sooner or later be widely recognised as third best compared to the ignored or suppressed vitamin D, other nutrients and early treatments.
How are the numerous vaccinophile individuals, officials and leaders going to cope with this truth?
If vaccine injuries and deaths really are much more extensive than is currently officially recognised (I feel they are to a significant degree, but I can’t quantify it) then how are governments and societies going to cope with the economic costs of the injuries and deaths themselves, the likely demands for financial compensation, and all the questions about responsibility and culpability which will arise?
U12 7th January 2022 - Critiques of the hypothesis that the excess deaths in 18 to 64 years olds can be attributed to a significant degree
I have no clear idea of what is going on here. However, I want to point to discussions which look interesting regarding the concerns many people have over ill-effects of COVID-19 mRNA and adenovirus vector “vaccines” causing death and disability in working age people in the USA to the extent that it shows up in significantly higher than normal deaths and claims for disability insurance payouts.
I did not think the comments at the TrialSiteNews copy of this article were particularly interesting. However several of the comments at the Rescue copy of Mary Beth Pfeiffer’s article struck me as significant: rescue.substack.com/p/chilling-pandemic-data-from-the-insurance/comments
Mary Pat Campbell has a Substack article concerning this potential excess mortality. She is a life actuary (actuary.org) so this is her field. The article marypatcampbell.substack.com/p/excess-mortality-for-working-age has graphs of US deaths by quarter, by age group.
Graph 3 shows higher overall change in deaths for most age groups for 2021 Q3 than for previous quarters, when compared to the quarter two years before. These are percentages of the deaths for each age group, +30% (for instance) for 35 to 44 years represents many fewer extra deaths than +30% for 75 to 84 year olds.
She states that (Graph 4) non-COVID-19 deaths of younger people in the USA, such as of 35 to 44 year olds, rose in 2020, before any COVID-19 vaccinations. She attributes this largely to a rise in drug deaths - a trend which predates COVID-19. Graph 6 shows death rates by different causal categories to May 2021, with COVID-19 deaths shown and with significant long-established growth in the “all other causes” and “accidental, suicide and homicide” categories. Graph 7 breaks down the latter category and shows that the growth is not largely due to homicide, suicide or transport accidents, but to “other external causes of accidental injury” - which (Graph 8) is growing almost entirely due to drug overdoses. Graph 9 shows that these deaths, and the growth in these deaths, is largely from people aged 25 to 64.
She argues that this worrying increase in deaths is due to drug overdoses, primarily of fentanyl and other opioids.Mary Beth Pfeiffer asks about heart attacks - not specifically mentioned in Mary Pat Campbell’s article.
Don Kress questions whether the deaths Scott Davison reports in people working for companies who took out insurance for them (I think this is what he was discussing) are not likely to be attributable to drug overdose, since employed people are less likely to abuse such drugs. He also questions whether drug overdose would lead to disability claims.
Marc Jolicoeur wrote: “COVID and overdoses need to be counted before jumping to conclusions that its vaccine related health issues. Also this pandemic has delayed health treatments and preventative care, increased depression, lowered physical activity, increase overeating, gaining weight, higher alcohol consumption, violent crime, and even speeding in cars. All of these also increased in 20/21.”
CPJ cites Australian data to October 2021 - the graphs of which I have looked at - and finds no overall increase in deaths. Deaths due to COVID-19 have been relatively small here compared those in many other countries. However, COVID-19 vaccination rates are very high, initially with AstraZeneca (adenovirus vector) and now with Pfizer and Moderna (mRNA, with the Moderna being similar to but stronger than Pfizer).
I have not tried to analyse this data further, but I regard it as a strong argument that whatever the cause of the worrying rise in deaths Scott Davison is referring to, it is unlikely to be largely due to COVID-19 vaccines, since Australia has higher rates of vaccination, with the same or similar vaccines, with much lower rates of drug overdose and deaths directly caused by COVID-19 - and I see no corresponding rise in deaths.
However, in late 2021 I did see some articles about hospitals here having unusually high numbers of non-COVID patients with heart and breathing problems. (I can’t find them in my thousands of COVID-19 bookmarks, but see The Standard article below.)Don Kress linked to an article which I did not read since it was very complex and I did not immediately ascertain that it was relevant to the current discussion.
thCnner cited a September 2021 US article, but the URL needed a www added: www.munichre.com/us-life/en/perspectives/group-and-living-benefits/examining-impact-covid-group-life-underwriting.html, stating that this shows similar trends to those reported for OneAmerica.
Maybe it does - there is a lot of detail here. However, to the extent it does, then the arguments just listed from Mary Pat Campbell and by the apparent (as best I can tell) non-appearance of such a trend in highly-vaccinated Australia, makes me provisionally conclude that the US death increases are not occurring in Australia, and so are unlikely to be caused to a large extent by the COVID-19 vaccination program.
The Australian data seems to argue against large-scale deaths from COVID-19 vaccines, at least in this country. However there are signs of ill-effects. I am particularly concerned about low-level, but widely experienced, ill-effects. It is no good looking up “shortness of breath” regarding the Pfizer vaccine because this is listed as a common side effect! Why would anyone want a “vaccine” which is supposed to act in their arm which somehow has even temporary ill-effects on their lungs???
There’s no way of knowing for sure which cells are being programmed to express the spike protein. I think it is mad to encourage or force whole populations - and especially children - to get any such treatment. (It might be justified due to protection against severe COVID-19 if there was no other approach, but vitamin D and early treatment provide much better protection and pandemic suppression, with no such safety problems.)
What if quite a few people lose one or a few percent of their lung capacity, for months or forever? Champion free diver Florian Dagoury lost his 30% of his diving performance after two Pfizer COVID-19 vaccine injections, according to his Instagram messages - and was diagnosed with myocarditis.
What if some of the rise in cardiovascular problems in the UK (Evening Standard 2021-12-14), with those aged 30 to 45 most at risk, are due to COVID-vaccine ill-effects, rather than the officially recognised cause of “post-pandemic stress disorder”, whatever that is? Some if it may be due to increased isolation and lack of medical care.
Tahir Hussain, a senior vascular surgeon at Northwick Park Hospital in Harrow, said he has seen a significant rise in cases where he works.
He said: “I’ve seen a big increase in thrombotic-related vascular conditions in my practice. Far younger patients are being admitted and requiring surgical and medical intervention than prior to the pandemic.
“I believe many of these cases are a direct result of the increased stress and anxiety levels caused from the effects of PPSD.
“We also have evidence that some patients have died at home from conditions such as pulmonary embolism and myocardial infarction. I believe this is related to many people self-isolating at home with no contact with the outside world and dying without getting the help they needed.”
~ ~ ~ ~ ~
I would be less concerned about reports of COVID-19 vaccine injuries if I thought that all medical professionals were responding properly to their incidence so the official account of these accorded with reality. However, I think the global pro-COVID-vaccine hysteria has many doctors and nurses in its grip.
Here is an interview with an Australian nurse (I have no idea of the location or source of the video, but I have kept a recording of it): twitter.com/Detrieman/status/1463825233257766914 .

She said:
. . . ED [Emergency Department] it really depends on who they get looking after them. I’d say the majority of doctors are pretty blind themselves and will swear black and blue that whatever they’re going through has nothing to do with the vaccine.
Depending on how severe, the odd doctor may say “Oh, this could be the vaccine.”.
You get a disgustingly healthy 30 year old guy, has not got any lung issues, cardiac issues - and he’s having acute chest pains, the constant feeling of pressure on his chest, shortness of breath, (???).
“Oh well maybe it could be from, you know, the second jab you got three days ago.”
- and so they will run tests.
In fact I had one doctor, I did blood tests on this guy, and I said “I reckon we should get a D-dimer [WP], which is a test to look for the presence of blood clots in the body”, and he’s like: “Oh, yeah - I guess we could do that.”
So I did the D-dimer and it came back and it was through the roof. It was like a thousand and it should be zero.
And he just turned to me and said: “You know I wish I had never taken that blood test.” . . . . .
I’m like “Well you have now, so you are obligated to do something about it.”.
So the blood test wouldn’t have been done. He would have gone home - and he could have died at home.
The interviewer asked: “Why did the doctor not want to take the blood test?”.
‘cause now he has to follow through and do all the tests. Whereas a lot of nurses in the background are like: “Oh, you know its just the same old, . . . People are assuming its the vaccine. There’s nothing wrong with the vaccine. He’s anxious, or he has anxiety or its all in his head.”.
This is what nurses are saying: “Its all in his head.”.
You don’t go to ED unless something is seriously wrong.
Similar reports of avoidant doctors can be found in this 2021-12-14 article from Ventura County, California: conejoguardian.org/2021/12/14/more-vc-nurses-blow-whistle-on-overwhelming-numbers-of-heart-attacks-clotting-strokes/
There are reports of neurological injuries as well:
Dr Been interview with Shaun Barcavage, a 51-year-old Research Nurse Practitioner from New York, who “has been struggling with the neurological issues since his [mRNA] vaccination”.
(Day 4 after first injection in right arm.) “I thought I had something stuck in my eye.” (Day 6) Flushed ear - bright red, for three days. Consulted a neurologist for the paresthesias. All subsided within 10 days of the first injection.
Second dose in late January 2021: Significant pain over three days radiated into his neck and back. “By day 4 I started to hear faint chime sounds in my right ear. Some of the tingling and right eye irritation returned. So even though I got the injection on the left, the flare of things started on the right again.”
He had no medical history, was healthy, had had numerous vaccines in the past with no ill-effects. He does not drink or smoke and was not using any medications or supplements. (This means his 25-hydroxyvitamin D levels were probably in the 10 to 20 ng/mL range, when his immune system needs 50 ng/mL to be healthy.)
“The tinnitus [WP] escalated to a severity which was profound. Like a 10 out of 10 where you’re literally on the bathroom floor and your crying because you can’t believe what has happened to you - and you thought this is not something you can live with. 1000% sure this is not coincidence.”
“Tachycardia [WP] wild swings in blood pressure and abdominal pain. I actually ended up in the the emergency department in Pennsylvania, tinnitus really bad, blood pressure 180/120, bad headache, tachycardia.” A CAT scan [WP] found some mesenteric inflammation (of the tissue that attaches the small and large intestines to the walls of the abdomen). He was sent home with ibuprofen. Steroids helped with the abdominal inflammation. He set up a tinnitus group online, which now has 3000 members. Diets didn’t help.
By March and April: tachycardia evolved into full-blown autonomic dysfunction, severe intractable insomnia, tachycardia episodes which would go for hours. “It was almost like my parasympathetic [WP] and sympathetic [WP] nervous systems would just not work. Every time my body wanted to go into calm, it would just trigger me. I would get (core?) adrenal dumps through my body which I could literally feel the chemical coursing through my body burning my stomach and muscles - this was by June/July.”
“I woke up one night in August with full-blown neuropathies, all over, generalised, my body stinging and my hands and feet burning.” Doctors did not help, but by July his neurologist was suspecting “pseudo-motor small-fiber” [WP] (neuropathy) - which was confirmed by skin biopsy. He had elevated cytokines immune system signaling molecules, some of which are pro-inflammatory. (This fellow probably has low vitamin D and so his immune system cannot work properly, and is more likely to have dysregulated inflammatory responses - see Chauss et al. at vitamindstopscovid.info/05-mds/.)
“Every day which passed by, I fear I slip more towards the chronic.”
“I may look healthy still, but I can assure you, when I sit here, my ears are hissing, my feet are burning and face’s nerve is taut, damaged. So I have a lot going on - and its not fun.”
“I get burn sensations down my chest. Feet feel sometimes like little toothbrushes on low vibration. Little prickling sensations everywhere. Burning. I feel nerve dysfunction in my hands when I stretch them - and I don’t know why.
Neither Shaun Barcavage nor Dr Been are anti-vaccination. This is not some poorly researched over-dramatised account. He tweeted a link to www.c19vaxreactions.com where you can read and view accounts of COVID-19 vaccine injuries collated by a group who are pro-vaccine. I sent him a message about vitamin D.
There are plenty of vaccine injury reports, such two interviews by John Campbell PhD (nursing) Neuro disease after vaccine with Nikk and a professional mountain biker. These items above are a small subset of what I could report if I went through all my bookmarks for the past few months, which would take several days to write-up.
This extensive 2021-12-15 article: thenationaldesk.com/news/health/we-do-exist-some-americans-suffer-life-changing-covid-vaccine-injuries describes several people’s broadly similar long-term - potentially permanent - complex, serious, injuries from COVID-19 vaccines:
Brianne Dressen, preschool teacher.
Shaun Barcavage, research nurse practitioner.
Cody Flint, crop-duster pilot (nearly blacked out when flying).
Joel Wallskog, orthopedic surgeon.
Suzanna Newell, former triathlete and long-distance biker.
Danice Hertz, retired gastroenterologist.
This interview is worth listening to: Dr Bryam Bridle, Associate Professor on Viral Immunology at the University of Guelph, on how mRNA vaccines can cause inflammation. He is one of the authors of this peer-reviewed article: Maternal COVID-19 Vaccination and Its Potential Impact on Fetal and Neonatal Development www.mdpi.com/2076-393X/9/11/1351.
THIS:
sc100ott
3 days ago
I’m a physician (radiologist) in the US. Every day I see CT scans of the chest for patients who come into Emergency with hypoxia. These are typically done to exclude the possibility of pulmonary embolism (PE). Most show no PE, but many show the extensive bilateral pneumonia pattern which is classic for CoViD-19. If I have a moment, I will check their medical record to see if there’s a Vitamin D level anywhere. For most patients there is no info, but maybe 1/4-1/3 do have a level from the past year or two. Invariably the patients with the worst disease have levels of 5-25, with most being 12 or less. I notice some have vitamin D listed on their medications, but usually only 1000 or 2000 iu per day. Not surprisingly, most of these patients are also obese. My story is only anecdotal. Working in a community hospital, I really don’t have any academic time to do a formal study, but I think there’s definitely a pattern which is important to acknowledge. Most of my colleagues want to pooh-pooh what I say, do I don’t feel like I can push too hard, unfortunately.
***** --- https://www.youtube.com/watch?v=w9h-XQm2qEY --- Is from comments at this YouTube video by a mainstream Doc. Very calm and competent fellow, Dr. John Campbell of Carlyle, England. He has a big youtube following
===
Please be wary of your sources re rowuhan matters.
From what I read so far, omicon is even milder than Delta. And some logically want it to let rip let to obtain community immunity.