


Early treatment with fluvoxamine, bromhexine, cyproheptadine, and niclosamide to prevent clinical deterioration in patients with symptomatic COVID-19: a randomized clinical trial
Yet health authorities, and many doctors, in the West are not interested.


This article does not directly concern nutrition. It focuses on the use of four repurposed drugs for treating COVID-19. These and other such drugs are systematically suppressed, at least regarding COVID-19 treatment, by the health authorities (and many doctors) in Western countries. These same authorities - and again a significant subset of doctors, together with academic journals and government efforts to restrict doctors work and public statements - also suppress the proper understanding and use of vitamin D3 and other nutrients to improve general health and to treat specific diseases.
Note 2024-03-19: I am not advocating the use of any of the drugs discussed below, starting with fluvoxamine, for treating COVID-19, except perhaps under medical supervision when a proper initial intervention involving calcifediol (or bolus vitamin D3), zinc, vitamin C, melatonin and ideally ivermectin has failed to bring about a clear recovery.
My interest in writing about this research is due to it showing (if the research is valid) that there are multiple inexpensive, well known, widely available drugs which are effective at treating COVID-19, beyond those just mentioned. Health authorities in the West ignore or try to suppress the use of all these, just as they do with vitamin D in general - see the next article on Dr Pierre Kory's experiences: nutritionmatters.substack.com/p/dr-pierre-kory-talks-with-tucker.
Anyone seriously interested in evaluating this research article and the use of fluvoxamine should read very widely. Please see the comments below and follow Tim Lunden's link to Anthony Colpo's multiple critiques. I also mention the strong warning the FLCCC doctors give regarding potential ill effects of fluvoxamine, including from a single dose.
[End of note.]
Fluvoxamine, AKA Luvox, (WP Wikipedia) is an SSRI (Selective Serotonin Reuptake Inhibitor) which is widely used as an antidepressant drug. It has some molecular and functional similarities to the better known fluoxetine (WP Prozac).
Early in the COVID-19 pandemic, some doctors noticed that hospitalised patients who were taking one or the other of these drugs suffered less severe COVID-19 symptoms than whose who took neither. (I don’t have the reference handy.) This may be due to the drugs’ anti-inflammatory effects.
Fluvoxamine has been the subject of a great deal of research: c19early.org/fmeta.html. However health authorities in Western countries have not approved it for use with COVID-19.
Steve Kirsch and other donors funded the first of the fluvoxamine RCTs (Randomized Controlled Trials), starting in April 2020: www.medpagetoday.com/special-reports/exclusives/91994.
He wrote in May 2022 kirschsubstack.com/p/how-the-fda-justified-rejecting-an about the United States Food and Drug Administration’s rejection of an application for fluvoxamine to be approved for emergency use for COVID-19.
This rejection is part of a corrupt and/or egregiously mistaken pattern of rejecting inexpensive, safe, well-known, drugs (and vitamin D3, which is a nutrient) in favour of the mRNA (Pfizer, Moderna) and adenovirus vector (Astrazeneca, J&J) quasi-vaccines, monoclonal antibody treatments (WP which are exceedingly narrow in the viruses they target, and so become rapidly ineffective as the viruses mutate) and expensive, not very effective, not very safe, profitable antivirals: Paxlovid (WP ) and Molnupiravir (WP).
Today Steve Kirsch reported kirschsubstack.com/p/new-thailand-randomized-clinical on a newly published article:
Early treatment with fluvoxamine, bromhexine, cyproheptadine, and niclosamide to prevent clinical deterioration in patients with symptomatic COVID-19: a randomized clinical trial
Wannigama and 20 other authors
BMJ eClinicalMedicine 2024-03-14
www.sciencedirect.com/science/article/pii/S2589537024000968
(This article does not contain the word “vitamin”.)
This RCT, conducted in Thailand between October 2021 and June 2022, involved 995 people who were diagnosed with COVID-19 and who did not, at time of diagnosis, need to be admitted to hospital. There were randomly divided into five groups. The first group of 336 patients received “standard care”. I am not sure what this was, but they were all at home, so this presumably did not involve any drugs or nutrients. The other four groups received this plus drug treatment for 14 days:
Fluvoxamine 100 mg/day, days 1, 2, 13 and 14, with 150 mg/day on days 3 to 12. (162 patients.)
Fluvoxamine plus bromhexine (WP) 16 mg/day for 10 days. (172 patients.)
Fluvoxamine plus cyproheptadine (WP) 12 mg/day for 14 days. (147 patients.)
Niclosamide (WP) 2 grams/day for 14 days plus bromhexine 16 mg/day for 10 days. (172 patients.)
18% of patients were infected with the early Alpha B.1.1.7 variant of the SARS-CoV-2 virus, 26% with Delta B.1.617.2 and the remaining 56% with an early Omicron variant B.1.1.529. The Omicron variants were more transmissible and less virulent - less likely to cause severe symptoms. These displaced all earlier variants in early 2022 in most or all countries.
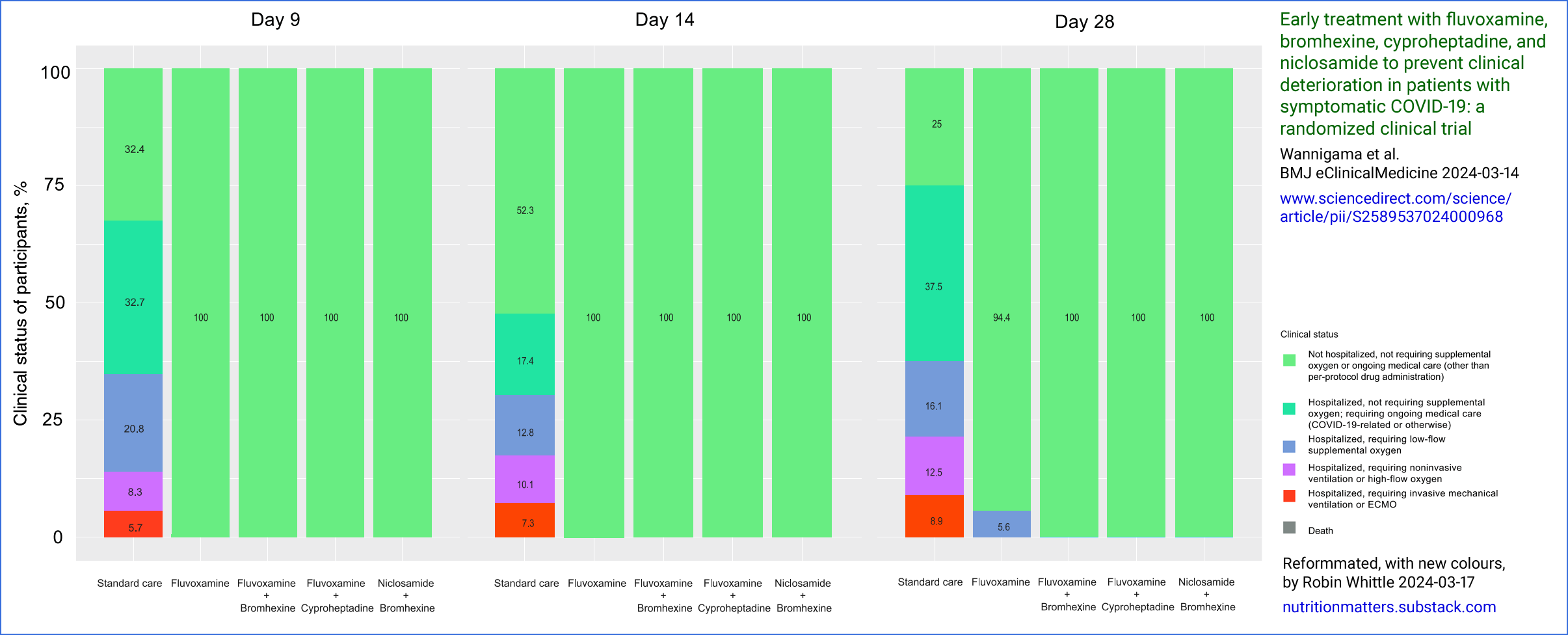
The results were stunning. The first chart, above, depicts the outcome on day 9: None of the treated patients needed hospital care, while 67% of the control group did, including 6.7% of these patients who needed intrusive mechanical ventilation (not just an oxygen mask) or ECMO (WP) - Extracorporeal membrane oxygenation, in which the lungs are not functioning and the patient relies on their blood being taken out continually to be oxygenated and have its carbon dioxide removed, and then returned to their circulation.
Here are the charts for days 14 and 28:


(These charts are reformatted, with more helpful colours, from the article’s Fig 2. If you would like the three combined: 5nn.info/temp/Wannigama-recolourised-all-days.png.)
{kind=link}
By day 28, nine patients in the fluvoxamine group required hospitalisation with low-flow supplemental oxygen. No other patients in the treatment groups required hospitalisation on any of these days 9, 14 or 28.
There was one severe adverse event in the treatment groups: a patient treated with fluvoxamine alone (0.6%). In the treatment group, 23 patients (6.8%) had serious adverse events. All these adverse events were: “loss of coordination with seizures/convulsions”. The percentage of patients in each group who had at least one non-serious adverse events were, 51.5% for the control group and 46.3%, 37.6% 29.3% and 27.3% in the four treatment groups.
These extremely positive results occurred without any attempt to measure or increase the typically very low 25-hydroxyvitamin D levels in the general population of most countries. See: nutritionmatters.substack.com/p/how-much-vitamin-d3-to-take and the research cited and discussed at: vitamindstopscovid.info/00-evi/.
The sections below contain some of the article’s description of the four drugs, with some text from their Wikipedia pages:
Fluvoxamine
A selective serotonin reuptake inhibitor (SSRI), is associated with benefit in the treatment of acute COVID-19 possibly by reducing damaging aspects of the inflammatory response to SARS-CoV-2 infection, lowering the risk of hypercoagulable state by reducing platelet serotonin levels, and/or other possible mechanisms. The initially hypothesized mechanism leading to clinical trials of fluvoxamine in COVID-19 was its anti-inflammatory action through activation of the sigma-1 (S1R) receptor [WP]. Fluvoxamine may also have antiviral effects through interaction with viral proteins and inhibition of acid sphingomyelinase.
Fluvoxamine, commonly sold under the brand names Luvox and Faverin, is an antidepressant of the selective serotonin reuptake inhibitor (SSRI [WP]) class. It is primarily used to treat major depressive disorder and obsessive–compulsive disorder (OCD), but is also used to treat anxiety disorders such as panic disorder, social anxiety disorder, and post-traumatic stress disorder.
Fluvoxamine's side-effect profile is very similar to other SSRIs: constipation, gastrointestinal problems, headache, anxiety, irritation, sexual problems, dry mouth, sleep problems and a risk of suicide at the start of treatment by lifting the psychomotor inhibition, but these effects appear to be significantly weaker than with other SSRIs (except gastrointestinal side-effects).
Although the many drug-drug interactions of fluvoxamine can be problematic (and may temper enthusiasm for its prescribing, advocation and usage to some), its tolerance-profile itself is actually superior in some respects to other SSRIs (particularly with respect to cardiovascular complications), despite its age.
Bromhexine
Bromhexine hydrochloride acts as a mucolytic and immune modulator to help clear chest congestion, and as a TMPRSS2 protease [WP] blocker may be an effective antiviral against SARS-CoV-2.
Bromhexine is a mucolytic drug used in the treatment of respiratory disorders associated with viscid or excessive mucus. It was developed in the research laboratory of Boehringer Ingelheim in the late 1950s as an active ingredient for pharmaceutical use, patented in 1961, introduced in 1963 under the trademark of Bisolvon® and came into medical use in 1966.
Cyproheptadine
Cyproheptadine acts as an antagonist of 5-hydroxytryptamine (5HT AKA serotonin [WP]) receptor subtype two [WP]. It is an immune modulator to prevent potent effects of serotonin on lung vascular tone, respiratory rate, and systemic vascular beds, which may potentially affect COVID-19 clinical outcomes.
It is sold under the brand name Periactin among others, is a first-generation antihistamine with additional anticholinergic, antiserotonergic, and local anesthetic properties.
It was patented in 1959 and came into medical use in 1961. In 2021, it was the 280th most commonly prescribed medication in the United States, with more than 800,000 prescriptions.
Niclosamide
The anti-helminthic [helminths (WP) are intestinal worms] drug niclosamide may be able to inhibit SARS-CoV-2 viral replication and modulate inflammation by markedly blunting calcium oscillations [calcium ion signaling of individual cells - I was not familiar with this and would need to read a tutorial such as cshperspectives.cshlp.org/content/12/1/a038802 to get up to speed] and membrane conductance in spike-expressing cells by suppressing the activity of TMEM16F [WP], a calcium-activated ion channel [WP], a scramblase [WP I had never heard of these either - they move phosphlipid molecules, which make up most of our cell lipid bilayer membranes [WP], between the inner and outer layers] responsible for the exposure of phosphatidylserine [WP] on the cell surface.
Niclosamide, sold under the brand name Niclosamide among others, is an antihelminthic medication used to treat tapeworm infestations, including diphyllobothriasis [WP tapeworms] , hymenolepiasis [WP tapeworms], and taeniasis [WP still more tapeworms]. It is not effective against other worms such as flukes [WP flatworms] or roundworms [WP nematodes]. It is taken by mouth.
Side effects include nausea, vomiting, abdominal pain, and itchiness. It may be used during pregnancy. It works by blocking glucose uptake and oxidative phosphorylation by the worm.
Niclosamide was first synthesized in 1958. It is on the World Health Organization's List of Essential Medicines. Niclosamide is not available for human use in the United States.
This study was the 42nd virus RCT on VitaminDWiki
https://vitamindwiki.com/tiki-index.php?page_id=15142
It includes charts comparing the effectiveness and costs of 20+ other treatments
- - - - One chart shows that the FDA only approved expensive treatments
I post a few of the 15,000 pages on VitaminDWiki.com on https://hlahore.substack.com
Dear Robin, it was good to see someone posting on fluvoxamine. My husband got Covid just before New Year's Day 2022. He spent some miserable hours in the ER New Years Eve due to an overzealous adult son being concerned about the oxymeter reading. The ER doctor sent him back home because there was "nothing in his lungs". This appeared in his electronic medical records which were seen by his practitioner who called me up to ask if we wanted an Rx for fluvoxamine for my husband. I said yes. The first pharmacy refused to fill it, so we used another pharmacy. It was a 10-day course. My husband spent a second week in bed sleeping through the day and night but then recovered somewhat quickly. It wasn't magic, but he did recover (73 yrs. old, TIA, replaced heart valve, sleep apnea). The interesting thing about this is that the physician and I had had a conversation about fluvoxamine 3 months before. He had seen its positive effects from the Together Study, and when I voiced concern about it being an SSRI, he had told me a 10-day treatment for Covid was not long enough for the side effects to show up.
On a later wellness exam in his office, he admitted to us that he was censured by his hospital review board for prescribing fluvoxamine. He was not ready to accept that, so went over their heads to the next higher up authorities (pharmacy board???) who told him the CDC committee that made the decision on whether fluvoxamine could be recommended for Covid treatment was split in a tie vote. When this board representative said we have to have a yes or no, the person on the other end said, well then, no! So, when our doctor went back to his own hospital system review board with this information, they removed the censure. Such politics! And most of us have no idea what is going on behind the scenes!