


IBS is caused by lack of vitamin D and intestinal worms
Irritable Bowel Syndrome and other inflammatory disorders can be suppressed with proper vitamin D3 supplementation and/or higher intakes than are normally required for immune system health.


Biologist Naomi Koh Belic PhD www.naomikohbelic.com wrote an Australian Broadcasting Corporation story www.abc.net.au/news/health/2022-11-11/ibs-irritable-bowel-syndrome-tiktok-hot-girl-stigma/101562030 with an accompanying Instagram video www.instagram.com/reel/CgOZxNVjfd3/ on Irritable Bowel Syndrome.
She improves vastly on the Hot Girl (Walk) meme established by influencer Mia on Tik Tok www.tiktok.com/@exactlyliketheothergirls/video/6933363802649955589 - and tells the world that she suffers from IBS.
There was no mention of vitamin D or helminths, so I established an Instagram account and wrote a suitably informative comment. However, I could not post it. I guess it was too long. It seems the Instagram comments system does not support well-referenced scientific discussion. Who knew??
Below is an illustrated and somewhat elaborated version of my comment. I will try to link to this article in a comment under the Instagram video.
A Google Scholar search for IBS and "Vitamin D" leads straight to Chong et al. 2022 Vitamin D supplementation for irritable bowel syndrome: A systematic review and meta-analysis: https://onlinelibrary.wiley.com/doi/full/10.1111/jgh.15852 which shows that vitamin D supplementation, well above the lousy 0.05 mg (200 IU) a day recommended by the 2006 Australian government guidelines www.eatforhealth.gov.au/nutrient-reference-values/nutrients/vitamin-d, significantly reduces IBS symptoms.
Such searches for all sorts of diseases, chronic health conditions and cancer lead to interesting research regarding vitamin D, since most people get so little that their immune system is crippled in-utero and from birth until their (frequently accelerated) death.
In research which should be known to every doctor, immunologist, virologist and public health official, Quraishi et al. 2014 jamanetwork.com/journals/jamasurgery/fullarticle/1782085 showed that the lower the pre-operative 25-hydroxyvitamin D AKA 25(OH)D level in the bloodstream was below 50 ng/mL 125 nmol/L (1 part in 20,000,000 by mass), the greater the risk of both post-operative surgical site infections and hospital acquired infections.

Above 50 ng/mL 125 nmol/L, the risk of each type of infection was about 2.5%. At 25 ng/mL 75 nmol/L - which is more than most Australians have in winter, unless they supplement vitamin D properly - the the risks rose to about 15% - a factor of 6.
This shows beyond reasonable doubt that innate and adaptive immune responses against bacterial pathogens are profoundly weakened by 25(OH)D levels below 50 ng/mL 125 nmol/L. 25(OH)D
is produced in the liver from ingested or ultraviolet-B created vitamin D3 cholecalciferol. It is the circulating compound that many types of immune cells need to supply their vitamin D based intracrine (inside each cell) and paracrine (to nearby cells) signaling system. The level of circulating 25(OH)D does not signal anything. It is not acting as a hormone. It is a raw material immune cells need, since they consume it when their vitamin D based intracrine/paracrine signaling system is activated.

(All medical professionals understand how 25(OH)D is used by the kidneys to produce a very low circulating level of 1,25-dihydroxyvitamin D, which acts as a hormone - a long-distance, blood-borne, signaling molecule - to control calcium-phosphate-bone metabolism. Some recognise, broadly, that “vitamin D” is important to the immune system - and may mistakenly assume that immune responses are affected by this very low level of 1-25(OH)2D.)
These vitamin D based intracrine (AKA, not quite accurately “autocrine”) and paracrine signaling systems are not related to hormonal signaling. The immune system does not use hormonal signaling. These two signaling systems play crucial roles in how each individual cell alters its behaviour in response to its changing circumstances. These signaling systems are activated by a different condition for each cell-type. When the system works, the changes to cell behaviour are, likewise, different for each cell type. You will frequently read that “vitamin D is a hormone” and that “vitamin D regulates immune responses”. For more on these mistakes - which are common even among people who write vitamin D research articles - please see Reinhold Vieth 2004 sci-hub.se/10.1016/j.jsbmb.2004.03.037, and: vitamindstopscovid.info/02-intracrine/#02-nothorm.
I have two hefty, recent (Janeways 9th) and current (Abbas 10th) edition, highly respected, immunology textbooks:
Many people, such as those with dark or black skin and/or sun-avoidant lifestyles have 25(OH)D levels below 15 ng/mL and sometimes as low as 5 ng/mL - a tenth of what their immune systems need to function properly. These disastrously low 25(OH)D levels - less than half of the 50 ng/mL 125 nmol/L the immune system needs - are normal in many countries, including Australia.
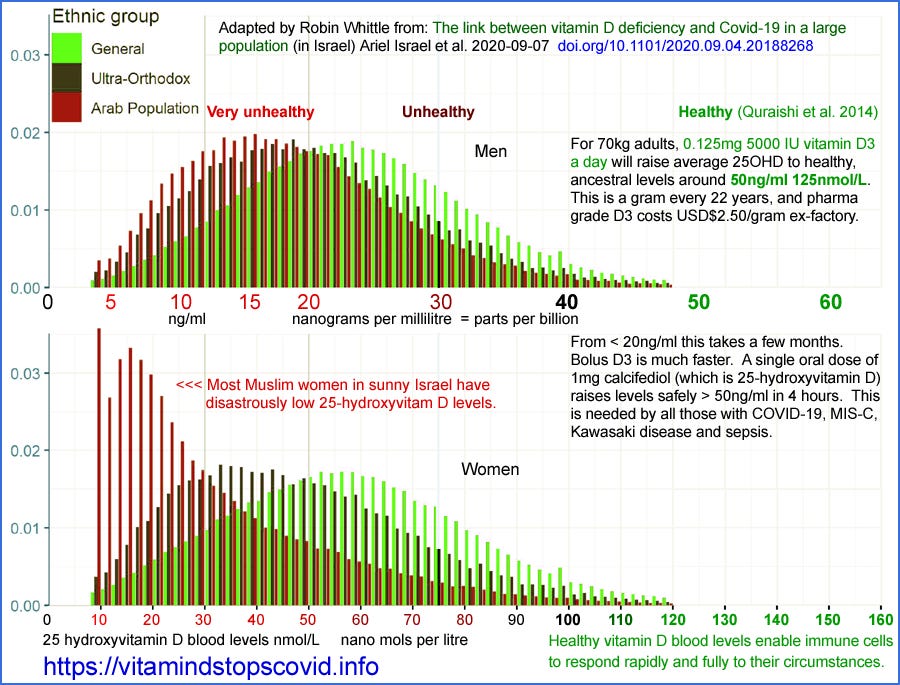
Even in sunny Israel, Arab (primarily Muslim, with typical all-covering clothing and sun avoidant lifestyles) have a median 25(OH)D level of about 12 ng/mL 30 nmol/L - 1/4 of what their immune system needs to function properly. (Israel et al. 2020 The link between vitamin D deficiency and Covid-19 in a large population www.medrxiv.org/content/10.1101/2020.09.04.20188268v1.)
In addition to weakened innate and adaptive responses, low 25(OH)D levels lead to excessive, self-destructive, indiscriminate cell destroying, dysregulated inflammatory responses. Chauss et al. 2021 www.nature.com/articles/s41590-021-01080-3 (my explanation of this dense cell-biology article: aminotheory.com/cv19/icu/#2021-Chauss) showed that Th1 regulatory lymphocytes from the lungs of hospitalised COVID-19 patients were unable to transition from their pro-inflammatory startup program to their anti-inflammatory shutdown program, even though the condition which signals (a high level of a complement [WP] protein) to do so was detected and so activated the cell's vitamin D based intracrine signaling system. The primary or sole reason this signaling system did not work, causing each Th1 cell to remain pro-inflammatory, was insufficient supplies of 25(OH)D.
IBS [WP], like numerous other autoimmune disorders, is caused by excessive inflammation. Inflammatory responses are primarily needed to defend against multicellular parasites, such as intestinal worms, AKA helminths [WP]. Humans were ubiquitously infested with helminths until about a century ago. Helminths long ago evolved to emit multiple compounds which downmodulate the inflammatory responses of their hosts - including those of our ancestors. Our ancestors evolved stronger inflammatory responses to counter this downmodulation. The same is true of most or all mammals.
Now, without helminths, our inflammatory responses are generally stronger than what is healthy for us. For genetic and other reasons (exposure to particular compounds or organisms) some people have such strong inflammatory responses that they suffer one or more of a vast array of chronic autoimmune inflammatory disorders, including IBS, Crohn's disease, psoriasis, rheumatoid arthritis, asthma etc.
This lack of helminths would cause some of these problems if everyone had the 25(OH)D they need, but most people have half or less of this. Most people's immune responses to bacterial, fungal and viral infections - and to cancer - are greatly weakened by low 25(OH)D levels, which also greatly exacerbates the proclivity to self-destructive inflammation.
So it is not surprising that helminthic therapy helminthictherapywiki.org - deliberately infecting oneself with a relatively benign species of helminths - suppresses IBS and many other inflammatory diseases. One 48 year old woman had "out of control fibromyalgia, IBS and rheumatoid arthritis" to the point where she "started picking out a new wife" for her husband. She wrote helminthictherapywiki.org/wiki/TSO_relieves_fibromyalgia,_IBS_and_rheumatoid_arthritis that introducing pig whipworm into her intestines "relieves fibromyalgia, IBS and rheumatoid arthritis".
It is also possible to suppress IBS and other such diseases, without helminths, by increasing 25(OH)D levels, as Chong et al. showed. The Coimbra protocol, for medically supervised 25(OH)D levels - typically much higher than 50 ng/mL 125 nmol/L - successfully suppresses the same set of diseases. See Amon et al. 2022: www.mdpi.com/2072-6643/14/8/1575 and, for Crohn's disease: coimbraprotokoll-de.translate.goog/2020/04/01/judi-sklerose/?_x_tr_sl=de&_x_tr_tl=en .
The vitamin D people tend to know nothing about helminths and the helminthic people tend to know nothing about vitamin D. Immunologists in general - and so most doctors - know nothing about either. They are much more interested in patented, and so profitable, drugs.
For more on the Coimbra protocol please see: coimbraprotokoll.de/en/scientific_principles/ and on vitamin D, helminths and excessive inflammation: vitamindstopscovid.info/06-adv/ .
There's very little vitamin D3 in food or multivitamins, so a "balanced diet" does not help. UV-B exposure of white skin can produce plenty of vitamin D3, but this is not generally available except in the middle of cloudless summer days with no sunscreen, glass or clothes covering the skin. The same UV-B always damages DNA and so raises the risk of skin cancer.
Supplements are the only practical way of attaining healthy 25-hydroxyvitamin D levels all year round. For 70 kg 154 lb bodyweight, without obesity, 0.125 mg 5000 IU a day will enable most people to attain this in about 3 months. This is a gram every 22 years - and pharma-grade vitamin D3 costs about USD$2.50 a gram ex-factory.
All sounds too simple? Please read the research cited in Prof. Sunil Wimalawansa's (CV) recent article in Nutrients www.mdpi.com/2072-6643/14/14/2997/htm and in my extensive page, with Patrick Chambers MD (see his work on vitamin D, magnesium and COVID-19): vitamindstopscovid.info/00-evi/ .
This includes a table which summarises Prof. Wimalawansa's body weight ratio based vitamin D3 supplemental intake recommendations: vitamindstopscovid.info/00-evi/index.html#sjw-updated-ratios . For people suffering from obesity, or chronic inflammatory conditions - including IBS - he recommends 90 to 140 IU per kg bodyweight vitamin D3 per day, on average. For 70 kg, this is 0.157 mg 6300 IU to 0.25 mg 10,000 IU per day.
Australian retailers are not allowed to sell capsules containing more than 0.025 mg 1000 IU vitamin D3. My wife Tina and I get 12.5 mg 50,000 IU capsules from Bio-Tech Pharmacal in the USA, who financially support two vitamin D researchers I know. These and 50,000 IU capsules from other companies can usually be obtained from Australian eBay sellers.

It is fine to take vitamin D3 every week to 10 days. I am 70 kg and take a one 1.25 mg 50,000 IU capsule once a week. This is 0.178 mg 7143 IU / day, plus 0.05 mg 200 IU / day from a multivitamin. At ex-factory prices, this capsule contains 1/3 of a US cent worth of vitamin D3 cholecalciferol.
I haven't bothered to get my 25(OH)D level tested. It is most likely between 60 and 100 ng/mL (150 and 250 nmol/L), which is fine with me.
I am an electronic technician and computer programmer who collaborates with vitamin D researchers in raising awareness of this terribly neglected nutrient, not least to reduce transmission and severity of COVID-19. My purpose in writing is to prompt you to read the research yourself. Don't take my word for any of the above.
Excellent article, the best I have ever read on D3.
TLDR