


Calcifediol (25-hydroxyvitamin D) or bolus vitamin D3 (cholecalciferol) are the only two vitamin D treatments for COVID-19
Ordinary daily D3 supplemental intakes raise 25-hydroxyvitamin D levels far too slowly. Calcitriol (1,25-dihydroxyvitamin D) doesn't help at all.

Much of the material below is covered by:

In general, please refer to this new article.
Ivermectin and “Vitamin D” are well known early treatments for COVID-19, but few understand how to raise 25-hydroxyvitamin D levels sufficiently in days or - ideally - hours
Dr Joel S Hirschhorn wrote a great article at TrialSite News (well worth USD$5 a month for anyone interested in health and medical research) concerning the terrible pattern of hospitals in the USA actively denying ivermectin treatment to seriously ill COVID-19 patients (2021-12-20):
trialsitenews.com/hospitals-choosing-patient-death-over-ivermectin/
An appreciative commenter described him as a “kind and compassionate doctor”, which indeed he is - though his 1965 PhD is in Material Science. The article concludes with a brief bio - and a fuller one can be found here.
Ivermectin is very well known among the growing number of healthcare professionals and interested non-medical people as a safe, effective ® early treatment for COVID-19. These people broadly know that vitamin D is likewise one of the most important early treatments. However, few seem to understand that only calcifediol or bolus (high, initial, dose) vitamin D3 cholecalciferol are effective. Ordinary daily D3 intakes or calcitriol are ineffective.
Here is a somewhat elaborated version of the comment I wrote to to Dr Hirschhorn’s article.
Thankyou Dr Hirschhorn for documenting this deadly and egregious abandonment of the purpose of medicine - care for the individual patient - in favour of clinicians and hospital administrators supporting a broader program of prioritizing vaccination above all else, with early treatment being treated as a dangerous distraction from that single, supreme, goal. Individual patients are made to suffer and die in order to promote the vaccines to the exclusion of all else program which is supposedly for the greater good. (The only exceptions are expensive treatments developed by multinational pharmaceutical companies.)
This is despite the demonstrated safety and effectiveness of ivermectin: ivmmeta.com, its success in the Indian state of Uttar Pradesh and recent research such as Kerr et al. 2021 (preprint).
Thanks too for your "Pandemic Blunder Newsletter" Substack: joelshirschhorn.substack.com .
Calcifediol (25-hydroxyvitamin D) or bolus (high initial dose) vitamin D3 cholecalciferol are the only two ways of using vitamin D compounds for early treatment of COVID-19
While ivermectin is an excellent early and late treatment for COVID-19, “vitamin D” is by far the most important and urgently needed treatment at any stage of COVID-19 - and likewise for sepsis [WP], Kawasaki disease [WP], Multisystem Inflammatory Syndrome [WP], ARDS (Acute Respiratory Distress Syndrome [WP]) and the common inflammatory disorder of pregnancy, pre-eclampsia [WP and Google Scholar].
Other early treatments include melatonin (non-prescription in the USA), quercetin (non-prescription in all countries), zinc, magnesium, vitamin C, B vitamins (especially B3): c19early.com and covid19criticalcare.com/covid-19-protocols/ .
I am using the term “vitamin D” to refer collectively to the three compounds:
Vitamin D3 cholecalciferol [WP].
25-hydroxyvitamin D calcifediol (AKA 25OHD and “calcidiol”) [WP].
1,25-dihydroxyvitamin D calcitriol [WP].
There are only two ways of achieving this for the great majority of the population who have not been supplementing vitamin D3 for months beforehand:
A single oral dose of ~1mg calcifediol - which _is_ 25-hydroxyvitamin D - (for 70kg bodyweight) or, if this is not immediately available:
Bolus [WP] vitamin D3 cholecalciferol such as up to 12.5mg 500,000 IU for 70kg bodyweight, without obesity. More is required in proportion to bodyweight for those suffering from obesity: aminotheory.com/cv19/obesity/ and vitamindstopscovid.info/01-supp/a-ratios/.
Both treatments will boost 25-hydroxyvitamin D levels above the 50ng/ml level required for proper immune system function. Calcifediol at 0.014mg / kg bodyweight will attain this in 4 hours while bolus vitamin D3 takes several days, due to the need for it to be hydroxylated to 25-hydroxyvitamin D in the liver. Both initial treatments should be followed by regular daily vitamin D3 to maintain the initially boosted 25-hydroxyvitamin D levels.
Calcifediol is now available without prescription in the USA and Australia, but it needs to be on-hand, ready to use - there is no point in waiting for it to be delivered. If calcifediol is not immediately available, bolus vitamin D3 is the best approach.
For more information on both early treatments, please see Professor of Medicine and long-time vitamin D researcher Sunil Wimalawansa (with whom I collaborate): www.linkedin.com/posts/sunilwimalawansa_multisystem-inflammatory-syndrome-mis-activity-6815294839769436160-99qJ/ and vitamindstopscovid.info/04-calcifediol/ .
Misunderstandings about the difficulty of raising 25-hydroxyvitamin D levels quickly and the role of hormonal 1,25-dihydroxyvitamin D
Two common misunderstandings are that an ordinary healthy daily intake such as 0.125mg 5000 IU vitamin D3 a day is adequate for a previously unsupplemented person who has been diagnosed with COVID-19, or that the patient should be treated with calcitriol (1,25-dihydroxyvitamin D).
For more on the calcitriol misunderstanding, and its ineffectiveness at treating sepsis: vitamindstopscovid.info/05-mds/#calcifediol-not-calcitriol.
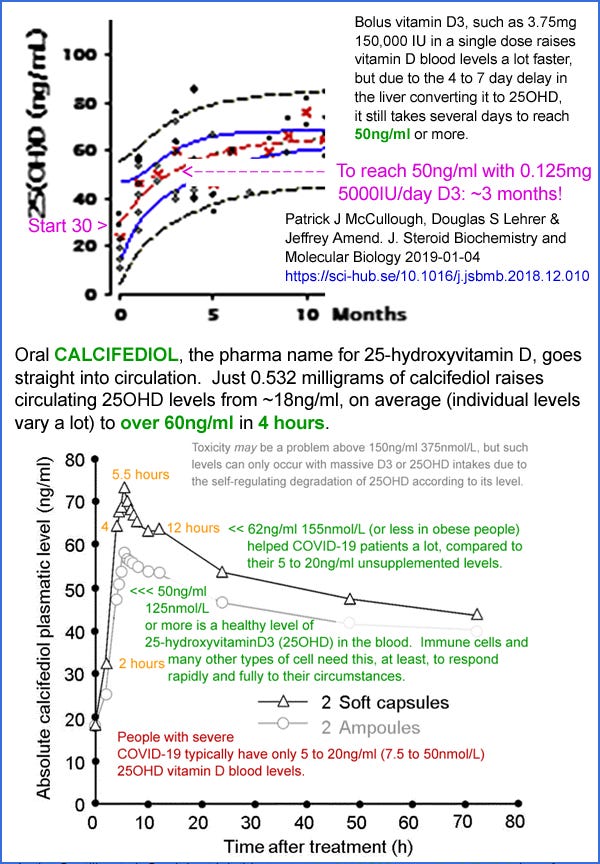
As you can see from the top graph at the start of this article, which is from Patrick McCullough et al. 2019, available at Sci-Hub, healthy daily D3 intakes such as 0.125mg 5000 IU / day (which are higher than what some MDs think is necessary, or even desirable) take months to raise 25-hydroxyvitamin D levels safely over 50ng/ml from typical un-supplemented baseline levels.
The red line (average, for these subjects in Ohio 40° north of the equator) in that graph starts at about 30ng/ml, which is a higher 25-hydroxyvitain D level than many people have, especially those with dark or black skin and/or whose clothing and lifestyle provides very little UV-B skin exposure and/or who live far from the equator (even the south of the UK is hell-and-gone from the equator: 52° north) and/or who are currently in winter or spring. All the more reason to take extra D3 to start with to boost levels much faster than the 3 or more months it would take with long-term healthy D3 intakes.
The bottom graph is from a patent for calcifediol capsules, which shows an average 4 hour 25-hydroxyvitamin D repletion time in healthy subjects who ingested 0.532mg calcifediol: patents.google.com/patent/WO2016124724A1/, from an average baseline level of ~18ng/ml. These test subjects were presumably in Spain.
Most people - and so most people infected with COVID-19 - have very low circulating 25-hydroxyvitamin D levels, such as 5 to 25ng/ml. 50ng/ml (125nmol/L) is the minimum required for proper immune system function. Immune cells need this level for their autocrine (inside each cell) and paracrine (to nearby cells) signaling systems to work rapidly and fully. My explanation of these signaling systems: vitamindstopscovid.info/02-autocrine/.
Individual immune cells largely rely on these signaling systems so that they can alter their behaviour to suit their changing circumstances. Their collective ability to respond rapidly and appropriately to change determines total immune system performance regarding strong innate and adaptive responses to pathogens and in better regulation of what may otherwise be overly-destructive inflammatory (cell destroying) responses.
See vitamindstopscovid.info/06-adv/ for research articles and discussion of how this proclivity to self-destructive overly-inflammatory responses arises, with considerable individual genetic variation, from us no longer being infected with helminths (intestinal worms), which exude compounds which downmodulate the inflammatory immune responses which target them. While two such compounds have been isolated and are being tested, no such compounds are yet available as drugs to suppress excessive inflammation in acute illnesses such as sepsis, severe COVID-19 etc. or for the very large number of auto-immune, inflammatory disorders such as psoriasis and rheumatoid arthritis, which can be suppressed by deliberate infection with helminths: helminthictherapywiki.org/wiki/index.php/Helminthic_therapy_personal_stories.
Please see the Chauss et al. 2021 regarding Th1 lymphocytes from the lungs of hospitalised COVID-19 patients being unable to transition from their pro-inflammatory startup program to their anti-inflammatory shutdown program - due primarily or solely to inadequate supplies of 25-hydroxyvitamin D. This is one of the research articles cited at: What every MD, immunologist, virologist and epidemiologist should know about vitamin D and the immune system: vitamindstopscovid.info/05-mds/ .
While many MDs consider 20ng/ml 25-hydroxyvitamin D to be adequate (see the history of this: vitamindstopscovid.info/01-supp/#iom), this is at best true for the 1,25-dihydroxyvitamin D hormonal regulation of calcium-bone metabolism. This is inadequate for the immune system. MDs and researchers have been calling for 40 to 60ng/ml 25-hydroxyvitamin D to be the standard of repletion since 2008: www.grassrootshealth.net/project/our-scientists/ . Quraishi et al. 2014 jamanetwork.com/journals/jamasurgery/fullarticle/1782085 showed that post-operative infections rose dramatically in proportion to how far below each patient's pre-operative 25-hydroxyvitamin D level was below 50ng/ml.

For a 70kg person to attain 50ng/ml or more 25-hydroxyvitamin D, on average, with considerable individual variation, 0.125mg 5000 IU vitamin D3 a day is required - and it takes 2 months or so to attain this from a typical baseline unsupplemented levels such as 5 to 25ng/ml.
There is very little vitamin D3 in food or multivitamins. Some foods are fortified with vitamin D2, which is not as effective as vitamin D3, and is present in quantities suitable for raising terribly low 25 hydroxyvitamin D levels (it is converted to a D2 version of this) to ~20ng/ml or so levels which greatly improves the regulation of calcium-bone metabolism.
UV-B skin exposure produces D3 but is not always possible, and damages DNA, which raises the risk of skin cancer.
In practice, for most people, the only way of attaining proper 25-hydroxyvitamin D levels is daily to weekly D3 supplementation in appropriate quantities, such as with the bodyweight ratio quantities suggested by Afshar et al. 2020 vitamindstopscovid.info/01-supp/#2020-Afshar - 70 to 100 IU / kg per day. Those suffering from obesity should use a higher ratio than this. (An IU of vitamin D3 is the amount a baby mouse needs per day to avoid the soft bone disease rickets [WP]. This is 1/40,000,000 of a gram, leading to scarily high IU numbers for ordinary healthy vitamin D3 daily intakes.)
So the great majority of the population is trying to live - and is now tackling COVID-19 - with a severely weakened and likely overly-inflammatory immune system, due to this easy-to-understand and easy-to-fix nutritional deficiency. The greatest and most perplexing problem we must solve is that most mainstream MDs remain oblivious to this global pattern of vitamin D deficiency. The great majority of health officials, physicians, immunologists, virologists and epidemiologists do not know this. I have two recent, highly regarded, epidemiology text books here - 1500 pages in all. Neither mention vitamin D in their indexes.
Immune cells are not affected by the very low, stable, level of circulating 1,25-dihdroxyvitamin D which acts as a long-distance blood-borne signaling molecule - a hormone. For a detailed explanation: vitamindstopscovid.info/02-autocrine/#02-nothorm.
The mistaken belief that the very low level of circulating, hormonal, calcitriol (1,25-dihydroxyvitamin D) must be boosted to improve immune system performance has lead to the Frontline Critical Care Consortium covid19criticalcare.com/covid-19-protocols/ recommending calcitriol and/or ordinary daily vitamin D intakes as preferred treatments for COVID-19. Hopefully their protocols will be corrected early in 2022 to recommend 0.014mg / kg single dose calcifediol or bolus vitamin D3. Update 2022-02-21: The I-MASK+ and I-RECOVER protocols were updated in January so neither recommends calcitriol.
In all other respects the protocols of the FLCCC - Dr Paul Marik, Dr Pierre Kory and their colleagues - for ivermectin, melatonin and other early treatments lead the world.
I believe that with immediate (4 hour or several day) 25-hydroxyvitamin D repletion, doctors following the FLCCC protocols will find their patients recovering quickly, and that they will need less or perhaps no corticosteroids (prednisone [WP]/ dexamethasone [WP]). These corticosteroids are a last-ditch method of suppressing deadly overly-inflammatory responses. However, they also weaken innate and adaptive responses to viruses and other pathogens, and boost blood glucose levels.
Please read the research articles I cite rather than rely on my opinions - I am an electronic technician and computer programmer. Medical advice is what you get from a healthcare professional working directly with you. Even if I was a doctor, I have not examined you!
Fantastic article and as someone that recently got COVID, i am grateful i had read this early enough. I got away with only 2 days of symptoms, no loss of taste symtom or any other left over. Plus ivermectin of course and the FLCCC protocol.
I've been looking for this exact information for a couple months now. Thank you SO MUCH for providing it and for all the links, as well.